Nasal passages and shells. Nasal passages. Nasal conchas. Clinical anatomy of the nose and paranasal sinuses
Outside, the nose consists of wings, or nostrils, the back of the middle part and the root located in the frontal lobe of the face. Inside its walls are formed by the bones of the skull, and from the side of the mouth it is limited to a hard and soft palate. It has a complex structure - the nasal cavity is divided into two nostrils, each of which has a medial (septum between the nostrils), lateral, upper, lower and back walls.
The sub-mechanical approach is of limited use in oncological surgery of the paranasal cavities. If endonasal removal of the test excision from the maxillary sinus fails, the antrum should be exposed through the anterior wall of the sublimation approach. These approaches may include very small tumors of the maxillary sinus. Unfortunately, such cases are rare in practice.
The name was based on the remote similarity of dragging the soft tissues of the middle of the face upwards with the removal of the glove. The incision is again in the lobby, but approximately centrally between the fangs. Another incision is round at the entrance to the nose on a bilateral basis. Then the soft tissue of the face is removed and raised up. This procedure is suitable for nasal tumors that cross the midline and maxillary sinus tumors.
In addition to bone tissue, the membranous and cartilaginous components of high mobility are included in the structure of the nasal cavity. There are three sinks in the cavity.- upper, middle and lower, but only the last true, since it is alone formed by an independent bone. The passages are located between the shells - the spaces through which the air flows:
The impact in the cranial part of the nasal cavity and in the cranial part of the olfactory cellars is limited. There are a number of changes in this section depending on the degree of exposure required. Distal can continue and cross the upper lip in the midline. From the cranial end, it can continue transversely in the lower eyelid or if orbital expansions are planned both in the eyelid and in the conjunctiva. Cranially, the cut may continue to search.
These approaches to the removal of soft tissues are followed by ablation rates. It is based on standardized procedures, but adapted to the extent of the tumor. Effective performance has been a general maxiectomy for centuries. This exercise involves resection of almost the entire upper jaw, including the patch plate. If a tumor spreads into orbit, orbital expansions are part of the operation. The second standard of today's work is maxelectomy in medicine, which involves resection of the side wall of the nasal cavity, mainly with a part of the olfactory labyrinth.
upper turn. It is located at the back and has openings in the cell of the ethmoid bone;
middle move It communicates with its frontal cells, with the frontal and maxillary sinuses;
lower turn. It connects through the nasal duct with the orbit.
The nasal cavity consists of the vestibule and the respiratory part.
The vestibule of the nose is lined with mucous membrane, which is composed of a multi-layered flat non-squaring epithelium and its own mucous plate.
Both versions have a number of modifications that take into account different clinical situations. This is basically a combination of neurosurgical procedure with the approach to the rhinologist. Sometimes this type of surgery is called a double-blind resection of the tumor. The neurosurgical approach is the most common bifunctional craniotomy. In addition, it is made extradural, after removing the side lobes, the degree of the process spreading to the front pit is clearly evaluated. The tumor is separated from the throat, eventually its part is resected and resection takes place at the base of the skull.
The respiratory part is lined with a single layer of multi-row ciliary epithelium. In its composition are distinguished:
ciliated cells - have ciliated cilia that oscillate against the movement of inhaled air, with the help of these cilia microorganisms are removed from the nasal cavity and foreign bodies;
goblet cells secrete mucins - mucus, which sticks together foreign bodies, bacteria and facilitates their excretion;
From the nasal approach, most often through lateral rhinotomy, the tumor is removed with a neurosurgeon from the front pocket. Another important step is the reconstruction of a defect in the cranial system. The reconstruction method depends on the size of the defect. It is almost always the pericranial lobe and tissue glue, often the fascia lata and large bone graft defects.
The nose, along with the eyes and mouth, is one of the most distinctive features of the face, which significantly affect our overall appearance. The nose is visible from the front and side, it is very often possible to determine, for example, by its size and shape, belonging to a particular ethnic group.
microvillous cells are chemoreceptor cells;
basal cells play the role of cambial elements.
The lamina propria of the mucosa is formed by a loose, fibrous, unformed connective tissue, in which simple tubular protein-mucous glands, vessels, nerves and nerve endingsas well as lymphoid follicles.
The nose and mouth serve as a gate for air to enter and exit the lungs. If we breathe calmly, the main air inlet is just a nose. But even during demanding exercises, when breathing becomes dominant, part of the air still passes through the nose. Despite the fact that the mouth is much larger, and we can take more air, a person is very uncomfortable if he has a stuffy nose and cannot breathe properly.
Nasal breathing is especially important for newborn babies who breathe almost exclusively through the nose. The unique configuration of their larynx allows them to breathe and suck at the same time without the risk of suffocation. Older children or adults do not control this — if they want to swallow, they should always stop breathing.
The mucous membrane lining the respiratory part of the nasal cavity has two areas that differ in structure from the rest of the mucosa:
the olfactory part, which is located on the greater part of the roof of each nasal cavity, as well as in the upper turbinate and the upper third of the nasal septum. The mucous membrane lining the olfactory region forms the olfactory organ;
Nose moisturizes the air we breathe
The nose is treated with inhaled air and its preparation for the reception of the larynx and lungs, which do not show dry air. Therefore, when inhaled air passes through the nose, it becomes moist and liquefies. Do you know why you have dry throatwhen you breathe for a long time? This is due to the fact that the air in the air is not moistened in the mouth.
Nose cleans the air you breathe
The air we breathe contains many things - in addition to oxygen and nitrogen - as well as dust particles, dirt, allergens, bacteria, viruses, and more. On the surface of the nasal tissue there are cilia that capture most of these impurities. Then they remain trapped in the mucus, which is slowly pressed into the throat, and then up to the stomach. Our stomach behaves much better than our lungs with adverse substances.
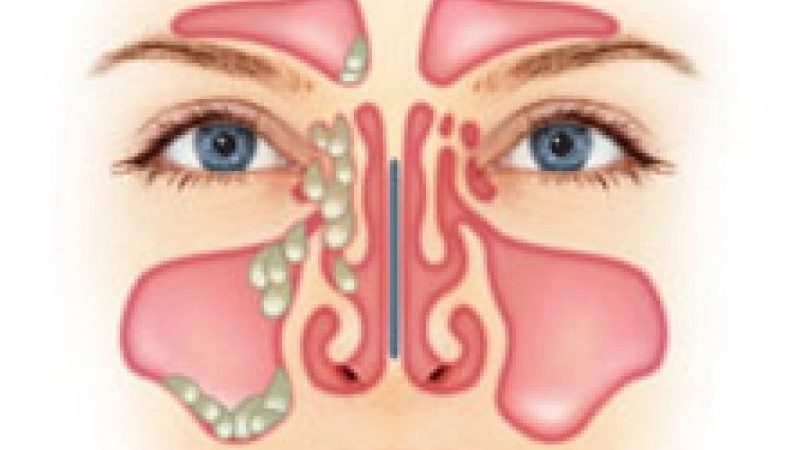
the mucous membrane in the region of the middle and lower turbinates differs from the rest of the nasal mucosa in that it contains thin-walled veins resembling the lacunae of the cavernous bodies of the penis. Under normal conditions, the blood content in the gaps is small, since they are in a partially collapsed state. With inflammation (rhinitis), the veins overflow with blood and constrict the nasal passages, making it difficult for nasal breathing.
Nose regulates the temperature of inhaled air
Just like our larynx and lungs, they do not like dirty air, they do not like too hot or too cold air. The passage of air through the nose allows the temperature of the inhaled air to be adapted to our body temperature, which is much better tolerated by mucous membranes. Cold air heating is much more common than warming, because people live mostly in places with colder temperatures than the temperature of the human body. You have already met with the so-called "nose" in cold weather.
The olfactory organ is the peripheral part of the olfactory analyzer. The composition of the olfactory epithelium includes three types of cells:
olfactory cells have a spindle shape and two processes. The peripheral process has a thickening (olfactory mace) with antennas - olfactory cilia that run parallel to the surface of the epithelium and are in constant motion. In these processes, upon contact with an odorous substance, a nerve impulse is formed, which is transmitted along the central process to other neurons and further to the cortex. Olfactory cells are the only type of neurons that have a precursor in the form of cambial cells in an adult individual. Thanks to the division and differentiation of basal cells, olfactory cells are updated every month;
This is a vivid example of heating and condensation of air that occurs in the nose in cold weather. The deep nose is an odor sensitive nerve cell. To smell and smell, we need to inhale inhaled air deep into the nose until these nerve endings. When we have rhinitis or allergies, the ability to suck air deep down to the olfactory receptors is limited. That is why our ability to smell is also limited.
But smell also plays a significant role in tastes. We distinguish four basic tastes: sweet, salty, sour and bitter. These tastes and all their variations, which we usually distinguish, are closely related to smell. This explains why during rhinitis or colds, there are not only bad smells, but also why we also tend to feel tasteless.
supporting cells are located in the form of a multi-row epithelial layer, on the apical surface have numerous microvilli;
basal cells have a conical shape and lie on the basement membrane at some distance from each other. Basal cells are undifferentiated and serve as a source for the formation of new olfactory and supporting cells.
Perception of aromas can be very pleasant, but the smell is also necessary for our safety! We need him to recognize, for example, smoke, spoiled food, or various toxic gases. People who have lost the ability to smell, should be much more attentive.
Nose modulates the sound of your voice
Last but not least, the sense of smell is also important for identifying people. Many people recognize their partner even after the smell, not only because of their body odor, but also because of the characteristic perfume or creams that the partner uses. What we hear when people talk or sing is largely dependent on the resonance in the throat and nose. A voice comes out of the larynx, but it's just a buzzing sound. The completeness of the sound is shaped by the way the sound is processed through the larynx, throat and nose. A particular voice in the cold, as it is called when someone speaks to the nose, is the result of a loss of resonance in the nose.
Axons of olfactory cells, vascular venous plexus, as well as secretory sections of simple olfactory glands are located in the lamina propria of the olfactory region. These glands produce protein secretion and secrete it to the surface of the olfactory epithelium. The secret dissolves odorous substances.
The olfactory analyzer is built from 3 neurons.
You can't talk about your nose without mentioning the nasal cavity. Cavities are air-filled structures that are located in the head of the face. One of their functions is that their head is “lighter”, but probably also played a significant role in raising a person. In addition, it performs the function of "airbag", which helps protect the brain and eyes.
The cavity, like the nose, is involved in voice modulation. In addition, they help control the level of nitric oxide in the body and lungs. It is incredible how much our body functions are focused on sexual activity and reproduction. Smell is one of the key components in which we identify people who are close to us. The characteristic smell of a partner’s perfume, the razor water or the smell of their shampoo or soap can be very significant in sexual arousal. The smell of human sweat even has a direct effect on sexual receptors in the brain.
The first neuron is the olfactory cells, their axons form the olfactory nerves and end in the form of glomeruli in the olfactory bulbs on the dendrites of the so-called mitral cells. This is the second link of the olfactory path. The axons of mitral cells form olfactory pathways in the brain. The third neurons are cells of the olfactory tracts, the processes of which end in the limbic region of the cerebral cortex.
Sense of smell is so associated with sexuality that the loss of smell leads to a decrease in appetite for sex. The main function of respiration is to provide every living cell of the body with oxygen, where it comes into contact with combustion, that is, the oxidation of nutrients. As a result of the oxidation process, the body is supplied with energy. As a result of changes in the cells, carbon dioxide is produced, which is released from the body by the lungs.
Lung oxidation, gas exchange and the subsequent removal of carbon dioxide are achieved through well-functioning respiratory organs. Nasal cavity is a double space at the beginning of the upper respiratory tract. The front nostrils and nostrils exit the entrance. Nasal cavities are bounded above by the nasal bone, the lead and the metal plate of the ethmoid bone; trinity, sacrum, harmony, power, sun, fruit, growth, development, meditation, happiness, consciousness.
The nasopharynx is a continuation of the respiratory part of the nasal cavity and has a structure similar to it: it is lined with a multi-row ciliated epithelium lying on its own lamina. The secretory sections of the small protein-mucous glands lie in the lamina propria, and the lymphoid tissue (pharyngeal tonsil) is located on the back surface of the lymphoid tissue.
Read more nasal passages producing nasal ducts. It is sent by the mucous membrane and multi-eyed epithelium. Epithelial function - air moistening, cleaning from pollution and heating. In the mucosa, there are goblet cells and a vesicular-follicular gland that secretes mucus. In the olfactory region, there is an olfactory epithelium containing olfactory cells.
The gulf is filled with air and connects with the nasal cavity, such as the frontal sinus, jaw. Paranormal ravines are cavities that connect with the nasal cavity. Paratroopers are even and differ in shape and size. There are sinuses, frontal, sagittal and wedge.
The structure of the paranasal sinuses.
The near-nasal sinuses consist of several parts that are interconnected.
The maxillary sinus is the air-cavity, adjacent to the nasal cavity and communicating with it by the maxillary orifice, which opens in the middle nasal passage. Okolonosovy sinuses to which also concerns maxillary sinus, in the form of primordia appear and embryonic period of fetal development; changing their shape and size, they continue to develop in the postnatal period and are finally formed at the age of 14–20 years.
The sky is the repository of the mouth, which consists of a hard and soft palate. The basis for the hard palate is palatal, palate and palatoplasty. Hard sky falls into the soft sky. Both arches and tongue form the shadow of the throat, which, thanks to the soft sky, can open and close. The throat is a wide muscular membrane about 12 centimeters long. This is the usual initial part of the respiratory and digestive tracts. It is made from flat muscles that tighten or lift the throat. The muscles are covered with a mucous membrane, which contains glands that produce slippery fluid, which reduces friction.
Maxillary sinus- the largest paranasal sinus. It is located in the thickness of the upper jaw and in form resembles a trihedral pyramid, the base of which is the external wall of the nasal cavity, and the tip is the zygomatic process of the upper jaw. The capacity of the sinus varies between 3-30 cm cubic, averaging 10-12 cm cubic. The air pressure in it is normally the same as in the nasal cavity.
The variability of the volume of the sinus due to the conditions of its development.
It was found that the maxillary sinus is formed due to resorption of the spongy substance of the upper jaw. It is possible that the chewing apparatus function influences this process. In cases where resorption occurs slowly and rather ends, the size of the maxillary sinus are so small that it can be taken as rudimentary; the walls of such a sinus are thick. Good bone resorption leads to the formation of a large sinus. According to German doctors, the narrowing of the maxillary sinus can also occur as a result of: 1) the convergence of the outer and inner walls of the sinus between themselves; 2) strong protrusion of the nasal wall and in the direction of the maxillary sinus; 3) thickening of the walls of the maxillary sinus; 4) tooth retention in the alveolar process; 5) combinations of all these conditions.
The inner wall of the maxillary sinus is the outer wall of the nasal cavity. This wall is the most difficult in the anatomical respect and has important clinical significance. It includes the nasal bones, the medial surface of the body of the upper jaw with the frontal process, the lacrimal bone, the cells of the ethmoid labyrinth, the perpendicular plate of the palatine bone and the inner plate of the pterygoid process of the main bone.
The inner wall of the maxillary sinus is mainly projected on the lower and middle nasal passages. Bone wall gradually thinning from the bottom up and from front to back and in the central part of the middle nasal passage is completely absent. Here the wall consists of a duplicature of the mucous membrane.
On the inner wall of the maxillary sinus at the base of the orbit there is a hole through which the maxillary sinus communicates with the nasal cavity in the area of the anterior section of the middle nasal passage.
The size of the hole is 2-19 mm in length and 2-6 mm in width. The hole located on the wall of the sinus does not correspond strictly to the mouth of the sinus in the nasal cavity and can be removed from it at a distance of 1 cm, resulting in an oblique canal. This circumstance in combination with the high position of the hole makes it difficult to outflow from the sinus. In some cases (10%) posterior to the first, main hole, there is a second, auxiliary, hole.
Through the maxillary hole air is exchanged in the sinus. Doctors have determined that with a normally functioning opening, the air in the cavity is exchanged by 90% for 5 minutes. The permeability of the maxillary opening is of great importance in the development of pathological processes in the sinuses.
The inner wall in the upper-posterior section is in close contact with the cells of the ethmoid labyrinth, which in some cases bulge into the sinus.
The upper wall of the maxillary sinus is the lower wall of the orbit. This is a thin bone plate, in which there are sometimes degiscension, covered with mucous membrane. In the thickness of this plate is the infraorbital canal, in which the same nerve, artery and vein pass. The channel in the form of a roller is contoured on the lower, sinus surface of the plate. Inogra in the specified cushion there are crevices and then the nerve and vessels passing in the canal are covered only with a thin mucous membrane, which should be considered when scraping the upper wall during sinus surgery.
The front, or facial, wall is the thickest, covered with soft cheek tissues and palpation is available. In the center of the front wall there is a groove - the canine fossa, which serves as a guide when opening the mandibular sinus. In this place the bone is the thinnest. At the upper edge of the canine fossa there is a hole through which the second branch goes to the surface. trigeminal nerve - infraorbital nerve. The back wall is bordered by the infratemporal and pterygo-pits, in the latter the pterygoid venous plexus is located.
The lower wall of the maxillary sinus is the posterior part of the alveolar process of the upper jaw. The bottom wall is in close contact with the holes of the first, second large molars and two small molars. In some cases, the bone tissue in the area of individual holes is absent and then the apex of the roots in contact directly with the mucous membrane of the bottom of the sinus. The lower wall of the middle maxillary sinus is at the level of the bottom of the nasal cavity, but is often located above or below the latter. According to the research data, the bottom of the maxillary sinus in 42.8% of cases is below the lower nasal passage, in 39.3% - on the same level with it and in 17.9% - above it.
Due to the close contact of the lower wall of the maxillary sinus with the roots of the teeth of the upper jaw, inflammation of the apex of the roots can cause inflammation of the maxillary sinus.
By the time of full development of the sinuses there are four cavities, or bays: alveolar, zygomatic, palatal and frontal. Often on the lower wall there are bony protrusions in the form of ridges, which partially, and in some cases completely, divide the sinus into two chambers. Partitions in the maxillary sinus can be either solid or with small holes. The formation of additional maxillary sinuses can also occur due to the ingrowth of one of the ethmoid cells. The capacity of these sinuses in adults ranges from 0.2 to 3.62 cm cube.
Of course, the presence of partitions that divide the sinus into separate parts, is of great practical importance, since due to them the disease can be unrecognized, and washing the sinus during puncture - difficult.
All anomalies of the maxillary sinuses can be detected on radiographs. Radiological abnormalities are detected in 13.3% of patients.
The suction capacity of the mucous membrane and the emigration of leukocytes are regarded as manifestations of the protective function of the shell of the paranasal sinuses.
Blood supply to the paranasal sinuses is provided by the branches of the internal and external carotid arteries, mainly through the orbital, external and internal maxillary arteries. The maxillary sinus feeds mainly on the posterior superior alveolar artery and the anterior superior alveolar arteries - the branches of the maxillary artery.
The outflow of blood from the paranasal sinuses is carried out through the vessels, which abundantly anastomose with each other, with the veins of the nose, face, orbit, and the cranial cavity, with cranial sinuses.
The venous system of the nose and paranasal sinuses is of great importance for the spread of infection.
Lymph outflow from the paranasal sinuses occurs to the deep cervical and pharyngeal nodes. The infection can spread through the lymphatic ducts to the deep sections of the neck and mediastinum.
The innervation of the paranasal sinuses is carried out by the first and second branches of the trigeminal nerve and the fibers of the pterygopalatine node.
In general, the maxillary sinus, like the other paranasal sinuses, protects the nerve structures of the orbit and the anterior cranial fossa from cooling and mechanical damage caused by breathing. In addition, the paranasal sinuses improve the respiratory function of the nose, serve to moisturize the nasal mucosa and perform the resonator function.
Not everyone knows that in the structure of the facial part of the skull there are hollow areas called nasal sinuses. The final formation of this part occurs by 5 years. The sinuses are connected with a special passage to the internal cavity of the nose.
Okolonosovy bosoms, have the different form and the sizes. They may change in the course of various previous diseases. Their inflammation passes with each person in different ways, taking into account individual physiological features.
Anatomy and function of the sinuses
Proper anatomical structure of the nose plays a big role in human health. Internal divisions also include everything. The anatomy of the nasal sinus is no less complicated and important than its functions, so it is worth considering this issue in more detail.
Due to the great importance of the sinuses, it is necessary to react as quickly as possible to the presence of fluid in them.
The main sinuses are referred to as wedge-shaped. This name they received due to its location in the sphenoid bone. Due to the fact that they border on other equally important parts of the body (pituitary, carotid arteries, ocular nerves), any inflammation is a great danger.
the biggest of all. They are located in the upper jaw. Each person has a different size. Each has recesses. The structure of the sinuses in its shape resembles a pyramid with three faces.
Inflammatory process in maxillary sinuses formed precisely in the fistula. Due to the fact that their lower part borders on the roots of the teeth of the upper jaw, very often any serious dental disease threatens with inflammation.
are in the frontal part above the eyebrows. They are connected to the nasal cavity with an anastomosis. Some people have additional partitions. It is interesting that not all people have frontal (frontal) sinuses, but about 95%. Full size, they reach only at the time of puberty.
Cells of the ethmoid labyrinth. They are located in the ethmoid bone, and their structure resembles interconnected cells that are different in size. Connect to the nasal cavity. The number of such cells reaches 15. The functions of the sinuses completely coincide with the basic functions of the nose.
Conclusion
Despite the fact that the entire system of smell has a rather complicated structure, they are multifunctional and are easily brought back to normal in almost any disease, if you catch it in time and start treatment.
In the event that time does not take up the treatment of diseases, the functioning of this system may be impaired, which would entail problems related to other functions of the body. Therefore, it is necessary to take action on time, together with a specialist.




Popular
- What is the name of the Scottish skirt
- What women like a man archer
- Dosage and use of doxycycline when tick bite
- Sinupret - complete instructions
- Number of antennae in arachnid and insect crustaceans
- Help for enterobiasis for the pool, how much is valid
- Ceftriaxone suspension. What is ceftriaxone?
- Third degree breast cancer: prognosis and treatment
- Salt Scrub for the scalp
- Do girls how many centimeters to the uterus