Shoulder anatomy. Brachial bone. Fracture of the humerus
There are many situations where a person can be injured. Sometimes this is not accompanied by a serious deterioration of the condition, but often it happens otherwise. This article will discuss such a problem as a fracture of the humerus.
Main
At the very beginning I want to say that bone fractures shoulder girdle make up about 7% of all such problems. Trauma can occur in any of its parts: diaphysis (middle), distal and proximal.
About bones
It is also worth saying that brachial bone refers to the section of long tubular bones. She has two ends:
- Distal. Located farther from the center of the body.
- Proximal. It is closer to the body. Consists of the so-called head and neck of the shoulder.
The bone itself is located between these ends.
Fracture classification
The name of the humerus fracture depends precisely on the site that is injured. At the same time distinguish:
- Proximal fractures. This is a trauma to the upper parts of the bone. It is worth saying that almost half of all fractures fall on this part.
- Diaphyseal. In this case, a fracture of the middle part of the bone occurs. Statistics say that it is this trauma accounts for 3% of all bone fractures.
- Distal fractures. In this case, the injury refers to the lower parts of the bone.

Causes of fractures
Why can the humerus break?
- Direct blow to the outer surface of the bone.
- Indirect kick - drop on the elbow.
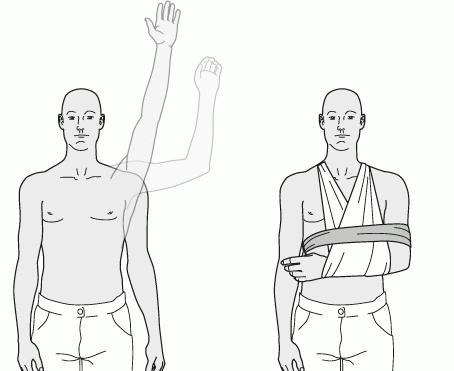
- Due to a fall on the elbow joint (adduction fracture) or on an outstretched arm (abduction fracture).
- Break the tubercle of the humerus can with the usual dislocation of the shoulder. Displacement can occur with contraction of the muscles of the shoulder girdle.
- Breaking humerus may due to injury.
Fracture Symptoms
If we are talking about a problem such as a fracture of the humerus, the symptoms will vary depending on the location of the injury. At the very beginning I want to talk about the signs of proximal fractures.
- Enlarged joint. In this case, it is customary to speak of edema or hemorrhage.
- Restriction of passive movement, active movements lead to severe pain.
- On palpation (palpation), the pain at the site of injury will increase significantly.

If the humerus was damaged in the area of the surgical cervix, the function of the joint will be possible, but still slightly limited. The pain will be localized in one place, significantly increasing during the load on the shoulder. If at the same time the humerus is also displaced, the person will feel acute pain when moving. The function of the joint will be impaired; pathological mobility is possible in the area of the fracture. Also with this type of trauma visually, the shoulder may become smaller.
If the tubercle of the humerus is fractured, the patient will show swelling. The functionality of the joint will be impaired, there will also be pain at the site of injury. because of pain sensations rotational and active movements will not be possible. Passive, in turn, will be very difficult.
If the humerus is broken in the diaphysal area, it can even be visually distinguished. So, shoulder deformation, its shortening will be looked through. Palpation will be a sharp pain, also strong pain will be observed at the time of tapping on the elbow.
When the bone breaks in the distal region, deformity of the lower third of the shoulder and elbow joint may be visible. During palpation, bone fragments will be palpable (above the elbow). Mobility in the elbow will be difficult due to pain. If the fracture occurs inside the joint, pathological mobility is possible with a crunchy sound (crepitus). May also occur with this type of fracture and complications. In this case, the rupture of the brachial artery or peripheral nerves is possible.
Diagnostics
In order to determine the diagnosis, the patient should go to the traumatologist’s appointment (as an alternative to the surgeon). Procedure Procedure:
- Collecting history.
- Palpation of the intended fracture site.
- Radiography in two projections.
Only on the basis of these indicators, the doctor will be able to make an accurate diagnosis and prescribe adequate treatment.
First aid
If there are assumptions that the bones of the shoulder girdle are broken, the patient should be given first aid. In this case, it will be relevant:
- Before the arrival of the ambulance, if necessary, the patient can enter analgesics. So, it may be such drugs as Novocain (injection), Nurofen, Diclofenac (tablets).
- The injured limb must be immobilized. You can impose a tire or at least fix the hand with a kerchief.
The person must be seated or put in such a way that there is no pressure on the injury site. Then you just need to wait for the arrival of an ambulance.

Treatment
Depending on exactly which bones of the shoulder girdle will be broken, treatment will also vary.
- If the proximal bone is broken, the treatment will be outpatient. An arm will be applied to the arm, and anesthetics (local anesthesia) will be injected into the joint. Later, physical methods will be needed, and a week later - gymnastics.
- If the surgical cervix is broken, the patient should be treated in the hospital. A closed response will be performed (the bone will be put in place in the event of an offset). Next, a thoracobrachial bandage will be applied (fixation of a bent elbow and a slight abduction of the arm back). From the very first days, the patient will be prescribed physiotherapy exercises for the hand and fingers, then work with the elbow. When the patient is able to keep his hand on the weight for at least half a minute, the Longuet will be removed. A full course of treatment is about two months.
- If the tubercles of the humerus are broken, then a Deso bandage will be applied. Full recovery will come in two months. If there was a displacement of debris, perhaps even surgery.
- If the humerus is fractured in the joint, a plaster longught with a bent elbow will be applied (for a period of about 1 month). If there was an intra-articular fracture with displacement, an extension will be required followed by the imposition of a U-shaped longuet.
As methods of physiotherapy, a patient may be prescribed a massage, therapeutic exercises. In some cases, shown magnetic therapy and UHF. When the gypsum is removed, it is possible to conduct ultrasound, electrophoresis with novocaine, ultraviolet irradiation.
ENCYCLOPEDIA OF MEDICINE / SECTION ^
ANATOMIC ATLAS
Humerus structure
The humerus is a typical long tubular bone that forms the proximal (upper) part of the arm. It has a long body and two ends, one of which articulates with the shoulder blade in shoulder joint, the other - with the ulnar and radial bones in the elbow joint.
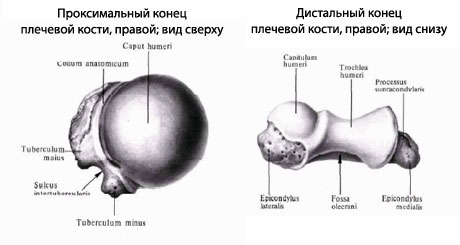
The tip of the humerus - its proximal end - has a large, smooth, hemispherical articular surface that articulates with the glenoidal cavity of the scapula to form the shoulder joint. The head is separated from the rest by a narrow interception - an anatomical neck, below which there are two bony protrusions - a large and a small tubercle. This tubercle serves as the site of attachment of the muscles and is divided by the intermontane furrow.
Body of the Shoulder Bone
_ (DIAFIZ) _
There is a slight narrowing in the upper body of the humerus — the surgical neck is a frequent fracture site. The relatively smooth surface of the diaphysis has two distinctive features. Approximately in the middle of the humerus body length, closer to its upper epiphysis on the lateral (lateral) surface, is the deltoid tuberosity, to which the deltoid muscle is attached. Below the tuberosity on the posterior surface of the humerus is a spiral groove of the radial nerve. In the deepening of this groove are the radial nerve and deep arteries of the shoulder.
The lateral edges of the diaphysis in its lower part become protruding medial (internal) and lateral inlays. The articular surface is formed by two anatomical structures: a block of the humerus, which is articulated with the ulna, and the head of the condyle of the humerus, which connects to the radius.
Humerus, back view
humerus
Articulated with the glenoid cavity of the scapula in the shoulder joint.
Anatomical -
It represents the rest of the growth zone, where in childhood bone growth occurs in length.
Body humerus
Diaphysis, is the main part of the length of the bone.
Radial nerve furrow
It passes obliquely along the back surface of the middle part of the body of the humerus.
Humerus block
Medial epicondyle -
More prominent bone outgrowth than lateral epicondyle.
Big knob
Place of attachment of muscles.
Humerus, front view
Small bump
Place of attachment of muscles.
Surgical neck
Narrow interception, frequent fracture site.
Deltoid tuberosity
Place of attachment of the deltoid muscle.
Head -
shoulder condyle
It has a spherical shape, articulated with the head of the radial bone.
Lateral epicondyle
External bone protrusion.
Anatomical neck
Inter-hill furrow
In it passes the tendon of the biceps muscle of the shoulder.
At these points, the bone is easy to feel under the skin.
Fractures of the humerus
Most of the fractures of the upper part of the humerus occur at the level of the surgical cervix as a result of a fall on the outstretched arm. Fractures of the humeral body are dangerous, possibly causing injury to the radial nerve lying in the groove of the same name on the back surface of the bone. Damage may cause muscle paralysis. back side forearm, which is manifested by drooping of the hand. H This radiograph shows a fracture of the upper body of the humerus. Such an injury usually occurs when falling on an outstretched arm,
In children, fractures of the humerus are often localized in the supra-shear region (in the lower part of the body of the humerus above the elbow joint). Usually the mechanism of such an injury is to fall on the arm, slightly bent at the elbow. It may damage nearby arteries and nerves.
Sometimes with complex fractures of the humerus, it becomes necessary to stabilize it with a metal pin that holds the bone fragments in the correct position.
Medial epicondyle
A bone protrusion that can be felt on the inside of the elbow.
Humerus block
Articulated with the ulna.
Humerus, humerus, is a long lever of movement and develops as a typical long tubular bone. According to this function and development, it consists of the diaphysis, metaphysis, epiphyses and apophyses. The upper end is provided with a spherical articular head, caput humeri (proximal epiphysis), which articulates with the articular cavity of the scapula. The head is separated from the rest of the bone by a narrow groove called the anatomical neck, the collum anatomicum. Immediately behind the anatomical neck there are two muscular hillocks (apophyses), of which the larger tuberculum majus lies laterally, and the other tuberculum minus lies a little anterior to it. Bone crests (for muscle attachment) go down from the tubercles: crista tuberculi majoris from the large tubercle, and crista tuberculi minoris from the small tubercle. A groove, sulcus intertuberculdris, is located between the two tubercles and the crests, in which the tendon of the long biceps head is placed. Immediately below both tubercles, the part of the humerus lying on the border with the diaphysis is called the surgical cervix - collum chirurgicum (the place of the most frequent fractures of the shoulder).
Body humerusin its upper part has a cylindrical shape, at the bottom is clearly triangular. Almost in the middle of the body of the bone on its lateral surface is tuberosity, to which the deltoid muscle, tuberositas deltoidea, is attached. Behind it, on the back surface of the body of the bone from the medial side to the lateral, a flat groove of the radial nerve, sulcus nervi radidlis, seu sulcus spiralis, passes in the form of a gentle spiral.
The extended and somewhat curved anteriorly lower end of the humerus, condylus humeri, ends on the sides with rough protrusions — medial and lateral crevices and epicondylus medialis et lateralis, which lie on the continuation of the medial and lateral edges of the bone and serve to attach muscles and ligaments (apophysis). The medial epicondyle is more pronounced than the lateral one, and on its posterior side it has an ulnar nerve sulcus, sulcus n. ulnaris. An articular surface is placed between the epicondyle for articulation with the bones of the forearm (dysgal epiphysis). It is divided into two parts: the so-called block, the trochlea, which has the form of a transverse roller with a notch in the middle, lies medially; it serves for articulation with the ulna and is covered by its cutting, incisura trochlearis; above the block, both in front and behind, is in the fossa: anterior coronary fossa, fossa coronoidea, posterior fossa of the olecranon, fossa olecrani. These pits are so deep that the bony septum separating them is often thinned to translucent, and sometimes even holed. Lateral to the block is placed the articular surface in the form of a segment of the ball, the head of the condyle of the humerus, capitulum humeri, which serves for articulation with the radius. In front of the capitulum is a small ray fossa, fossa radialis.
Ossification.By the time of birth, the proximal epiphysis of the shoulder is still composed of cartilage, therefore, on the radiograph of the shoulder joint of a newborn, the head of the shoulder is almost undetectable. In the future, there is a consistent appearance of three points:
- in the medial part of the head of the shoulder (0-1 year) (this bone nucleus may be in the newborn);
- in the large tubercle and lateral part of the head (2-3 years);
- in tuberculum minus (3-4 years).
These nuclei merge into a single head of the humerus (caput humeri) at the age of 4-6 years, and synostosis of the entire proximal epiphysis with diaphysis occurs only at the 20th-23rd year of life. Therefore, on radiographs of the shoulder joint, belonging to children and young men, are marked according to the indicated ages of enlightenment at the site of the cartilage, which separates the parts of the proximal end of the humerus that are not yet merged from each other. These enlightenments, representing normal signs age changesshould not be mixed with cracks or fractures of the humerus.
Which doctors should be asked to examine the Shoulder bone:
Traumatologist
What diseases are associated with the Shoulder bone:
What tests and diagnostics need to be done for the Shoulder bone:
X-ray of the humerus
Is something bothering you? Do you want to know more detailed information about the Shoulder bone or do you need an inspection? You can make an appointment with the doctor - clinic Eurolab always at your service! The best doctors they will examine you, advise, provide necessary assistance and make a diagnosis. you also can call a doctor at home. Clinic Eurolab open for you around the clock.
How to contact the clinic:
The telephone number of our clinic in Kiev: (+38 044) 206-20-00 (multichannel). The secretary of the clinic will pick you a convenient day and time of the visit to the doctor. Our coordinates and directions are indicated. Look in more detail about all the services of the clinic at its.
If you have completed any research be sure to take their results to a consultation with a doctor. If the studies were not performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You must be very careful about your overall health. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, they are already too late to heal. To do this, just need several times a year. be examined by a doctor, not only to prevent a terrible disease, but also to maintain a healthy mind in the body and the body as a whole.
If you want to ask a question to the doctor - use the online consultation section, maybe you will find the answers to your questions and read self care tips. If you are interested in reviews about clinics and doctors - try to find the information you need at. Also register on the medical portal. Eurolab, to be constantly updated with the latest news and updates on the Shoulder bone on the site, which will be automatically sent to you by mail.
Other anatomical terms starting with letter "P":
| Esophagus |
| Chin |
| Spine |
| Navel (navel) |
| Penis |
| Prostate |
| Crotch |
| Liver |
| Parathyroid glands |
| Pancreas |
| Bud |
| Medulla |
| Pleura |
| Peripheral nerves |
| Webbed labyrinth |
| Podgolovaya cavity |
| Oral cavity |
| Rectum |
| Plasma |
| Vertebrae |
| Lumbar vertebrae |
| Shoulder joint |
| Groin area |
| Shoulder |
| Forearm |
| Finger |
| Peripheral nervous system |
| Parasympathetic nervous system |
| Sweat gland |
| Gonads |
| Prostate |
| Placenta |
| Appendix ovary and periolic |
| Paraganglia |
| Right ventricle |
| Cardiac conduction system |
| Atrioventricular node |
| Pericardium |
| Shoulder head |
| Subclavian artery |
| Axillary artery |
| Brachial artery |
| Popliteal artery |
| Anterior tibial artery |
| Shoulder veins |
| Anterior jugular vein |
| Subclavian vein |
| Vertebral venous plexus |
| Right lymphatic duct |
| Isthmus of the rhomboid brain |
| Forebrain |
Humerus, humerus, is a long lever of movement and develops as a typical long tubular bone. According to this function and development, it consists of the diaphysis, metaphysis, epiphyses and apophyses. The upper end is provided with a spherical articular head, caput humeri(proximal epiphysis), which articulates with the articular cavity of the scapula. The head is separated from the rest of the bone by a narrow groove, called anatomical neck, collum anatomicum. Immediately behind the anatomical neck are two muscular hillocks (apophyses), of which bigger tuberculum majuslies laterally and the other smaller tuberculum minusa little anterior to it. From cusps, bone ridges go down (to attach muscles): from a large cusp - crista tuberculi majoris, and from small - crista tuberculi minoris. Between both bumps and ridges passes groove sulcus intertubercularisIn which is placed the tendon of the long head of the biceps. Immediately below both tubercles, the part of the humerus lying on the border with the diaphysis is called surgical neck - collum chirurgicum (the place of the most frequent shoulder fractures). The body of the humerus in its upper part has a cylindrical outline, at the bottom is clearly triangular. Almost in the middle of the body of the bone on its lateral surface is tuberosity, to which is attached deltoid muscle, tuberositas deltoidea. Behind her on the back surface of the body of the bone from the medial side to the lateral passes in the form of a gentle spiral flat radial nerve sulcus, sulcus nervi radialis, seu sulcus spiralis.
Extended and slightly curved anteriorly lower humerus end, condylus humeri, ends on the sides of rough protrusions - medial and lateral epicondyle and, epicondylus medialis et lateralis, lying on the continuation of the medial and lateral edges of the bone and serving to attach the muscles and ligaments (apophysis). The medial epicondyle is more pronounced than the lateral one, and on its back side has ulnar sulcus, sulcus n. ulnaris. An articular surface is placed between the epicondyle for articulation with the bones of the forearm (dysgal epiphysis). It is divided into two parts: medially lies the so-called block, trochleawhich has the form of a transverse roller with a notch in the middle; it serves to articulate with the ulna and is covered by its tenderloin, incisura trochlearis; above the block, both in front and behind, is in the fossa: in front coronary fossa, fossa coronoidea, behind the fossa olecranon, fossa olecrani. These pits are so deep that the bony septum separating them is often thinned to translucent, and sometimes even holed. Lateral to the block is placed the articular surface in the form of a segment of the ball, the head condyle humerus, capitulum humeriused for articulation with the radius. Front over capitulum is small fossa radialis.
Ossification. By the time of birth, the proximal epiphysis of the shoulder is still composed of cartilage, therefore, on the radiograph of the shoulder joint of a newborn, the head of the shoulder is almost undetectable.
In the future, there is a consistent appearance of three points: 1) in the medial part of the head of the shoulder (0 - 1 year) (this bone nucleus may be in the newborn); 2) in the large tubercle and the lateral part of the head (2 - 3 years); 3) in tuberculum minus (3 - 4 years). These nuclei merge into a single head of the humerus (caput humeri) at the age of 4–6 years, and synostosis of the entire proximal epiphysis with diaphysis occurs only at the age of 20–23. Therefore, on radiographs of the shoulder joint, belonging to children and young men, are marked according to the indicated ages of enlightenment at the site of the cartilage, which separates the parts of the proximal end of the humerus that are not yet merged from each other. These enlightenments, representing normal signs of age-related changes, should not be confused with fractures or fractures of the humerus. Ossification of the steel end of the humerus, see the description of forearm bone ossification.
Shoulder fracture - a fairly common injury, during which there is a violation of the integrity of the humerus.
Fracture of the humerus in facts and figures:
- According to statistics, a shoulder fracture is 7% of all other types of fractures (according to various sources, from 4% to 20%).
- Trauma is often found among both the elderly and young people.
- A typical mechanism for the occurrence of a fracture is a drop on an outstretched arm or on the elbow.
- The severity of the fracture, the nature and timing of treatment depends strongly on what part of the shoulder is damaged: upper, middle or lower.
Features anatomy of the humerus
The humerus is the long tubular bone, which is connected to the scapula (shoulder joint) by the upper end, and the lower end to the bones of the forearm (elbow joint). It consists of three parts:- upper - proximal epiphysis;
- middle - body (diaphysis);
- lower - distal epiphysis.
 The upper part of the humerus ends with the head, which has the shape of a hemisphere, a smooth surface and articulates with the articular cavity of the scapula, forming the shoulder joint. The head is separated from the bone by a narrow part - the neck. Behind the neck are two bony protrusions — a large and a small tubercle, to which muscles are attached. Below the tubercles is another narrow part - the surgical neck of the shoulder. This is where the fracture most often occurs.
The upper part of the humerus ends with the head, which has the shape of a hemisphere, a smooth surface and articulates with the articular cavity of the scapula, forming the shoulder joint. The head is separated from the bone by a narrow part - the neck. Behind the neck are two bony protrusions — a large and a small tubercle, to which muscles are attached. Below the tubercles is another narrow part - the surgical neck of the shoulder. This is where the fracture most often occurs. The middle part of the humerus, its body, is the longest. In the upper part it has a round cross-section, and in the lower - triangular. A furrow spirals along the body and around the humerus; it contains the radial nerve, which is important for the innervation of the arm.  The lower part of the humerus is flattened and has a large width. There are two articular surfaces on it, which serve for articulation with the bones of the forearm. On the inside is a humerus block - it has a cylindrical shape and articulates with the ulna. On the outer side there is a small cap of the humerus, which has a spherical shape and forms a joint with the radius. On the sides at the bottom of the humerus are bone elevations - external and internal namyshchilki. Muscles are attached to them.
The lower part of the humerus is flattened and has a large width. There are two articular surfaces on it, which serve for articulation with the bones of the forearm. On the inside is a humerus block - it has a cylindrical shape and articulates with the ulna. On the outer side there is a small cap of the humerus, which has a spherical shape and forms a joint with the radius. On the sides at the bottom of the humerus are bone elevations - external and internal namyshchilki. Muscles are attached to them.
Types of humeral fractures
Depending on the location:- a fracture in the upper part of the humerus (head, surgical, anatomical neck, tubercles);
- body fracture of the humerus;
- fracture in the lower part of the humerus (block, cap, internal and external namesake).
- intra-articular - a fracture occurs in the part of the bone that takes part in the formation of a joint (shoulder or elbow) and is covered with an articular capsule;
- extraarticular.
- no bias - easier to treat;
- with displacement - the fragments are displaced relative to the initial position of the bone, they must be replaced in place, which is not always possible without surgery.
- closed - skin is not damaged;
- open - there is a wound through which fragments of bone can be seen.
Fractures in the upper part of the humerus
 Types of fractures in the upper part of the humerus:
Types of fractures in the upper part of the humerus:- head fracture - it can be crushed or deformed, it can break away from the humerus and turn around 180 °;
- fracture of the anatomical neck;
- fracture of the surgical neck - fractures of the anatomical and surgical neck of the shoulder are most often impacted when one part of the bone enters the other;
- fractures, tears of large and small tubercle.
The reasons

- drop on the elbow;
- a blow to the upper shoulder;
- tears of the tubercles most often occur in the shoulder joint, due to a sharp strong contraction of the muscles attached to them.
Symptoms of upper arm fractures:

- Swelling in the shoulder joint.
- Hemorrhage under the skin.
- Sharp pain.
- Depending on the nature of the fracture, movement in the shoulder joint is not possible at all or partially possible.
Diagnostics
 The victim must be immediately taken to the emergency room, where he is examined by a trauma doctor. He feels the area of the damaged joint and identifies some specific symptoms:
The victim must be immediately taken to the emergency room, where he is examined by a trauma doctor. He feels the area of the damaged joint and identifies some specific symptoms: - When tapping on the elbow or pressing it, the pain increases significantly.
- During palpation of the joint area, a characteristic sound appears, resembling bursting bubbles - these are the sharp edges of the fragments that touch each other.
- The traumatologist takes the victim’s shoulder with his own hands and carries out various movements. At the same time, he is trying to feel with his fingers which parts of the bone are displaced and which remain in place.
- If at the same time as a fracture there is a dislocation - when palpating the shoulder joint, the doctor does not detect the head of the shoulder in its usual place.
Treatment
 If there is a bone fracture or fragments are not displaced, usually the doctor simply performs anesthesia and applies a plaster cast for 1-2 months. It starts from the scapula and ends on the forearm, fixing the shoulder and elbow joints.
If there is a bone fracture or fragments are not displaced, usually the doctor simply performs anesthesia and applies a plaster cast for 1-2 months. It starts from the scapula and ends on the forearm, fixing the shoulder and elbow joints. If there is an offset, before applying the plaster cast, the doctor performs a closed reposition - returns fragments to the correct position. Most often this is done under general anesthesia, especially in children.
On the 7-10th day, physical therapy (movements in the elbow, wrist, shoulder joint), massage, physiotherapy treatment are started
| Procedure | Purpose | How is it done? |
| Novocain electrophoresis | Elimination of pain. Anesthetic penetrates directly through the skin into the joint area. | For the procedure, use two electrodes, one of which is located on the front surface of the shoulder joint, and the other on the back. The electrodes are wrapped with a cloth moistened with a solution of the drug substance. |
| Calcium chloride electrophoresis | Reduction and inflammation, acceleration of bone regeneration. | |
| UV - ultraviolet irradiation | Ultraviolet rays contribute to the release of biologically active substances in tissues, contribute to the strengthening of regeneration processes. | Opposite the shoulder joint is placed a device that generates ultraviolet radiation. The distance from the device to the skin, the intensity and duration of irradiation are selected depending on the sensitivity of the skin. |
| Ultrasound | Ultrasonic waves carry out tissue micro-massage, improve blood flow, enhance regeneration processes, provide an anti-inflammatory effect. Ultrasonic irradiation is completely safe for the body. | Use a special device that generates ultrasonic waves. It is directed to the area of the shoulder joint and carry out irradiation. |
All these procedures are not applied simultaneously. For each patient, the doctor draws up an individual program, depending on his age, condition, availability associated diseases, severity of fracture.
Indications for surgical treatment for fractures of the humerus in the upper part:
| Type of operation | Indications |
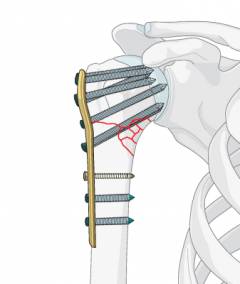 |
|
Fixation of fragments using steel spokes and wire.  | In elderly people with osteoporosis of the bones. |
Fixation with a steel screw.  | Hind bone tubercle with displacement, rotation. |
Endoprosthetics - replacement of the shoulder joint with an artificial prosthesis. 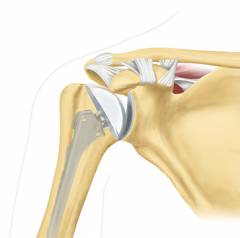 | Severe damage to the humeral head when it is split into 4 or more fragments. |
Possible complications
Dysfunction of the deltoid muscle. Occurs as a result of nerve damage. The paresis, - partial disturbance of movements, - or full paralysis is noted. The patient can not take his shoulder to the side, raise his hand high.Arthrogenic contracture - impaired movement in the shoulder joint due to pathological changes in it. The articular cartilage is destroyed, the scar tissue grows, the joint capsule and ligaments become excessively dense, lose their elasticity.
Habitual dislocated shoulder - A complication that develops after a fracture (when a fracture and dislocation occur simultaneously). If the treatment was carried out incorrectly or out of time, then in the future dislocation arises easily, from a minor effort.
Fracture of the humerus in the middle

The reasons





Popular
- What is useful mineral water
- What is the name of the Scottish skirt
- What women like a man archer
- Dosage and use of doxycycline when tick bite
- Sinupret - complete instructions
- Number of antennae in arachnid and insect crustaceans
- Help for enterobiasis for the pool, how much is valid
- Ceftriaxone suspension. What is ceftriaxone?
- Third degree breast cancer: prognosis and treatment
- Salt Scrub for the scalp