The occipital bone of a newborn is sticking out. Features of the structure of the skull of the newborn. Age changes of the skull
CHE PE P IN C EOLOM
Newborn skull
The skull of a newborn has the following characteristics: 1) the shape and size of the skull, the ratio of its parts are significantly different from the skull of an adult (Fig. 1); 2) the number of bones is greater than that of an adult; 3) significant layers of webbed connective tissue and cartilage are observed between the bones of the roof and the base of the skull.
The skull of a newborn is very elastic, since numerous parts of the bones are connected to one another by layers of connective tissue. This feature undoubtedly facilitates the adaptation of the fetal head to the pelvic bone-fibrous ring of a woman during labor, when the margins of the parietal bones are centered on each other, as well as the scales of the frontal and occipital bones on the parietal bones. As a result, the inter-dark and anteroposterior diameters decrease and the longitudinal size of the head increases. The skull of the newborn has a dolichocephalic shape. The head circumference is 34 cm, the volume in boys is 375-380 cm. Cube, in girls - 350-360 cm. Cube.
Fig. 1. Proportional relations of the skull of the newborn and adult (according to A. Andronescu).
And - the newborn; B is an adult.
NEWBORN SKULL DIMENSIONS
The distance between the bumps of the parietal bones is 9.5 cm. The distance between the external auditory canals is 8 cm. The occipital-frontal size is 11.5 cm. The occipital and mental size is 13 cm.
From these dimensions, it follows that during labor the head should not pass through the birth-chin size through the birth canal, otherwise complications arise.
When examining the skull of a newborn in front (Fig. 1), there is a significant development in the cerebral part of the skull compared to the facial part, which is 65% of the length of the head. The facial skull is short and wide, the orbits are well developed in it. This is due to the fact that the eyeball and the auxiliary apparatus of the eye are well developed and prepared for the perception of light stimuli. The upper jaw, having a primordium of the pneumatic sinus and devoid of the alveolar process, of small size. This in turn has an impact on the size of the nasal cavity and nasopharynx, which are presented in the form of a narrow slit. Only with the inclusion of the act of sucking and breathing increases the function of the muscles, which, together with food and air, has a formative effect on the bones of the skull.
The cranial cavities differ markedly from the cranial cavities of an adult. Bone outer auditory canal absent and the drum cavity with auditory ossiclesenclosed in connective tissue
are under the skin.
The orbit has the shape of a triangular pyramid, the entrance is round, its diameter is 25-27 mm (35-40 mm for an adult). The upper and lower orbital fissures are wide open. Between the bones that form the orbit, there are visible layers of connective tissue. Due to the poor development of the orbital
the ethmoid bone wall is weakly expressed.
The nasal cavity is represented by a slit with a height of 18 mm and a width of 7 mm at the level of the lower nasal passage, at the level of the top - a width of 3 mm (in an adult, respectively, 54, 15 and 10 mm). With the middle nasal passage the rudiment of the upper jaw air-bearing sinus is reported. Other sinuses and ethmoid cells
bones are missing.
Pterygium fossawell expressed, has a message with five wide channels.
The temporal fossa is limited on the medial side by the scales of the temporal bone and the large wing of the sphenoid bone. The depth of the fossa at the level of the zygomatic process is 12 mm, in an adult it is 2 times larger, although other sizes of the skull of an adult exceed the size of the skull of a newborn by several times. This indirectly indicates that large and well developed masticatory muscles are located in the temporal fossa.
Many bones of the skull of a newborn, presented in an adult in the form of one bone, consist of separate parts. This feature can be explained not only by the fact that such a mosaic skull is more easily adapted to the shape of the birth canal, but also by the fact that it repeats its phylogenetic development. In all animals below man, there is a greater number of bones in the skull. The fusion of bones in the skull of an adult is due to the need to protect the hemispheres of the brain.
Between the individual bones and their parts there are large layers of webbed connective tissue and cartilage, called fontanelles. The layers between the bones on the base of the skull are filled with cartilage.
The newborn has six springs (Fig. 2). Outside, they are covered with skin and aponeurosis of the head, on the side of the cranial cavity adjacent to them dura mater. In the area of the springs, there is a pulsation of the arteries of the brain and membranes, which is why these areas are called pulsating, gushing. The size and size of the springs are subject to significant fluctuations, depending on the rate of ossification of the bones of the skull. By the time of closing the fontanels you can judge the mineral metabolism and assess the physical development of the child.
1. Front fontanel(fonticulus anterior) unpaired, usually diamond-shaped, 3.5 x 2.5 cm in size. Limited by scales. frontal bone and two parietal bones. Replaced with bone by the end of the 2nd year of life.
2. The rear fontanelle (fonticulus posterior) unpaired, is located between
shuya occipital bone and corners of the parietal bones, has a triangular shape with a length of 1 cm. The final closure is observed by the end of the 2nd month
after birth.
3. Wedge shaped spring(fonticulus sphenoidalis) paired, irregular rectangular shape, 0.8 x 1.2 cm in size. Limited by the edge of the anterior lower angle of the parietal bone, by the scales of the frontal and temporal bones, large
the wing of the sphenoid bone.
4. Mastoid springwell(fonticulus mastoideus) doubles, slightly less than the previous one. Unlike other fontanelles closed cartilage. It is located between the lower posterior angle of the parietal bone, the scales of the temporal and occipital bones. Wedge-shaped and mastoid springflowers close at 3 months after birth.
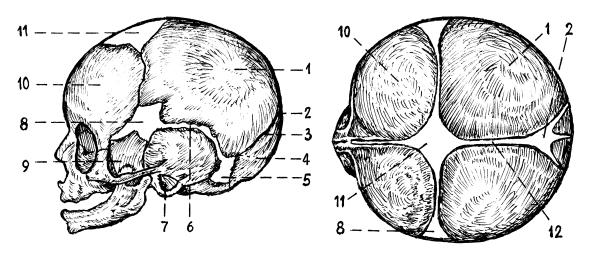
Fig. 2. The skull of the newborn. Side and top view (by Morris):
1 - parietal bone; 2 - rear fontanel; 3 - fabric layer for lambdoid seam; 4 - occipital bone; 5 - mastoid spring; 6 - scaly seam; 7 - drum ring; 8 - wedge-shaped spring; 9 - a large wing of the sphenoid bone; 10 - frontal bone; 11 - front fontanel; 12 - sagittal suture.
There are more additional springs that close in the first days after birth (Fig. 3).
On the basis of the skull distinguish interlayers filled with cartilage:
1) layer of the steam room, limited to the pyramid of the temporal bone and the lateral parts of the occipital bone, filled with fibrous cartilage;
2) the steam room is located between the top of the pyramid and the body of the sphenoid bone;
3) cartilaginous layer between the body of the sphenoid and occipital bones. As a result, a slope is formed;
4) cartilaginous layer between the separate parts of the occipital bone.
FEATURES OF THE STRUCTURE OF THE SUPPORT-MOTOR SYSTEM IN CHILDREN.
Features of the structure of the skeleton of the trunk and limbs in childhood.
The bone system of the newborn is characterized by the presence of a large number of cartilage tissue, the reticular structure of the bones, in which the gaversov channels have an irregular shape, a rich vascular network in the neck of the bone (areas with large proliferative development), a considerable thickness of the periosteum. The weight of the cartilage and bones that make up the skeleton is 15-20% of the total body weight. The process of skeletal ossification begins with the appearance of ossification nuclei in connective tissue and cartilage models of bones. The nuclei of ossification that appear in intrauterine life are called primary nuclei, and those that appear after birth are secondary. The entire skeleton develops with the appearance of 806 nuclei of ossification.
The sequence of nucleation of ossification is hereditary, but the time of appearance and the speed of their development depend on a number of factors: ethno-territorial, gender, social conditions. Usually in girls the time of appearance of ossification nuclei and their development occurs earlier than in boys. In infancy, the difference in the time of appearance of ossification nuclei is approximately 1 week, in children under 5 years of age it is a year or more. In the long tubular bones, ossification of the diaphysis occurs in the prenatal period. By the time of birth, ossification points may appear in distal epiphysis femur and proximal tibial epiphysis, which is a sign of full-term fetus. Further, ossification points appear in the apophysis, the metaphysis is the last to ossify, which indicates the end of skeletal growth.
The newborn in the skeleton is only 28 g. Sa, at the one-year-old one it increases 3 times, at 18 years old - 1035 g. Sa.
Features of the skull of the newborn.
The skull of a newborn is relatively large. The facial section is much smaller than the cerebral (ratio 1/4, in an adult - 1/2). Dominance brain department associated with the rapid development of the central nervous system (brain) in the prenatal period. Underdevelopment of the alveolar process, the absence of teeth, underdevelopment of the paranasal sinuses and the nasal cavity in general, the smoothed relief of the bones of the facial skull cause the smaller dimensions of the facial skull.
In the bones of the skull roof there is a large amount of connective tissue. The edges of the bones are even, the gaps between them are filled with connective tissue, which creates the relative mobility of the bones to adapt the head to the birth canal (the phenomenon of konoriguration). In the corners of the parietal bone, connective tissue is retained in the form of fontanelles. Mastoid and styloid fontanelles are small, and normally close by the time of birth (or the first month after birth), occipital - in the first half, frontal has a diamond shape, large sizes are closed in the second year of life. The skull of a newborn has the appearance of a pentagon, since the parietal, occipital, and frontal cusps are well expressed (primary ossification points of the integuinal bones of the skull).
A large amount of cartilage tissue is preserved in the bones of the skull base, which in the postnatal period ossifies and remains as temporary and permanent synchondrosis. The mastoid cells are in their infancy, their permanent formation goes to the 3rd year.
Skullfrom the moment of birth to the end of life undergoes great changes.
The skull of a newborn has the following characteristics:
1) the shape and size of the skull, the ratio of its parts are significantly different from the skull of an adult (Fig. 73).
2) the number of bones is greater than that of an adult;
3) significant layers of webbed connective tissue and cartilage are observed between the bones of the roof and the base of the skull.
The skull of a newborn is very elastic, since numerous parts of the bones are connected to one another by layers of connective tissue. This feature undoubtedly facilitates the adaptation of the head of the fetus to the pelvic bone fibrous ring of a woman during labor.
When examining the skull of a newborn in front (Fig. 73), there is a significant development of the cerebral part of the skull as compared with the facial skull is short and wide, in which the orbits are well developed. This is due to the fact that the eyeball and the auxiliary apparatus of the eye are well developed and prepared for the perception of light stimuli. The upper jaw, having a primordium of the pneumatic sinus and devoid of the alveolar process, of small size.
The cranial cavities differ markedly from the cranial cavities of an adult. The bone tissue of the external auditory canal is absent and the tympanic cavity with the auditory ossicles, enclosed in the connective tissue, is located under the skin.
The orbit has the shape of a triangular pyramid, the entrance is rounded
Pterygopal fossa is well expressed, has a message with five wide channels.
The temporal fossa is limited on the medial side by the scales of the temporal bone and the large wing of the sphenoid bone. The depth of the fossa at the level of the zygomatic process is 12 mm, in an adult it is 2 times larger, although other sizes of the skull of an adult exceed the size of the skull of a newborn by several times.
Between the individual bones and their parts there are large layers of webbed connective tissue and cartilage, called fontanelles. The layers between the bones on the base of the skull are filled with cartilage.
The following springs are distinguished:
front fontanel, fonticulus anterior, diamond-shaped, located in the midline at the intersection of four seams: sagittal, frontal, and the two halves of the coronal; overgrown in the 2nd year of life;
rear fontanel, fonticulus posterior; triangular in shape, located at the posterior end of the sagittal suture between the two parietal bones in front and the scales of the occipital bone in the back; overgrown on the 2nd month after birth;
lateral fontanelles, paired, two on each side, with the anterior called sphenoid, fonticulus sphenoidalis, and posterior called the mastoid, fonticulus mastoideus. The cuneiform spring is located at the point of convergence of the angulus sphenoidalis of the parietal bone, frontal bone, large wing of the sphenoid bone, and scales of the temporal bone; overgrown in the 2-3rd month of life.
The mastoid spring is between the angulus mastoideus of the parietal bone, the base of the pyramid of the temporal bone and the scales of the occipital bone. Wedge-shaped and mastoid springs are observed more frequently in premature babies, and in the full-term, the occipital can sometimes be absent. In newborns, there is a lack of sutures, poor development of diploy, non-expression of relief, not only on the outer, but also on the inner surface of the skull. The remains of the second cartilaginous stage of development of the skull are the cartilaginous layers between the separate parts of the base bones that have not yet merged, which therefore are relatively larger in the newborn than in the adult.
Age differences of the skull in general, its topographic areas and individual bones are expressed primarily in various ratios of brain and facial departments. These differences, as well as the thickness of the bones, the size of the pits and cavities of the skull, the presence of fontanelles and synostosis of the sutures of the skull, etc., are determined by the growth and development of the skull. There are 5 periods of development of the skull. The first period - from birth to 7 years - is characterized by an active growth of the skull, an intensive increase in its volume. At the same time, the seams are slightly narrowed and the value of springs, fonticuli. The nasal and orbital cavities are shaped; relief changes noticeably lower jaw. In the second period - from 7 to 14 years - the change in the size and shape of the skull and its parts is not as active as in the first, but the fossa, mastoid, the cavity of the orbits and the nose increases markedly. The third period covers the age from puberty to 25 years. At this time, the frontal regions are formed and lengthened. facial skull, the area of the zygomatic arches increases markedly, the frontal cusps protrude more. During the fourth period, from 25 to 45 years, the ossification of the sutures occurs. Observations have shown that premature ossification of the arrow-shaped suture leads to the formation of short, and the coronal suture leads to the formation of long skulls. The fifth period - 45 years and more - is characterized by facial atrophy, and then brain skull, a gradual decrease in the number of teeth, which affects the shape of the jaws: the alveolar processes and parts are smoothed, the angle of the mandible increases, the facial skull is reduced in size.


Popular
- Breast cancer is curable at any stage.
- The remedy for the cold Sinupret
- Azitrox - official instructions for use
- Chicken-bjaka: allowed antibiotics were found in Russian chicken
- Oral Cancer: Symptoms and Treatment
- Dark and thick blood during menstruation.
- Modern analogues of doxycycline tablets
- Is it possible to die from pneumonia
- What earwax will tell all about your health
- Tussin: instructions for use