Nasal sinuses structure. Nasal cavity. Its structure and functions
Nasal cavity(cavitas nasi)is the beginning of the respiratory system. It is located under the base of the skull, above the mouth and between the sockets. The front of the nasal cavity communicates with the external environment through
nasal openings - nostrils (nares),back - with the nose of the pharynx through the rear openings of the nasal cavity - choans(choanae).Nasal cavity formed by bony walls covered with mucous membrane. With the nasal cavity connected paranasal sinuses.The mucous membrane of the nasal cavity extends into the paranasal sinuses.
Nasal septum(septum nasi)the nasal cavity is divided into two halves - the right and left. In each half, distinguish nasal vestibule(vestibulum nasi),limited to cartilages of the external nose and covered with multilayered flat epitheliumand the nasal cavity itself, lined with mucous membrane with a multi-row ciliated epithelium. The boundary between the vestibule and the nasal cavity passes along the arcuate comb - the nasal threshold (litep nasi).
In the nasal cavity 4 walls: upper, lower, lateral and medial. Medial wallcommon to both halves of the nasal cavity, is represented by a septum of the nose. There are 3 parts of the nasal septum:
1) upper bone (pars ossea);
2) anterior cartilaginous (pars cartilaginea);
3) anteroposterior membranous (pars membranacea).
At the front edge of the opener is a coulom-nasal organ. (organum vomeronasale),representing a complex of small folds of the mucous membrane. In humans, this organ is small, functionally related to the sense of smell.
Bottom wallthe nasal cavity is also the upper wall of the oral cavity. On the bottom wall, posterior to the coulone-nasal organ, the incisal duct (channel) is located (ductus incisivus),opening a hole on the incisive papilla of the palate.
It is important for dentists to keep in mind the relation of the roots of the upper incisors to the lower wall of the nasal cavity. In some people, especially those with a wide and short face, the tops of the medial upper incisors and the upper canine are very close to the bottom of the nasal cavity, being separated from it only by a thin layer of compact jaw substance. On the contrary, in persons with a narrow, long face, the tips of the roots of the upper incisors and canines are removed from the nasal cavity for a considerable distance (10-12 mm).
Top wallor vault of the nasal cavity, formed by the cribriform plate of the ethmoid bone, through which the olfactory nerves pass, therefore the upper part of the nasal cavity is called olfactory region(reg. olfactoria),as opposed to the rest of the cavity - respiratory area(reg. respiratoria).
Lateral wallhas the most complex structure. On it are 3 turbinates: the upper, middle and lower (conchae nasales superior, media et inferior),the core of which is the corresponding osseous nasal concha. The mucous membrane of the shells and the venous plexuses embedded in it thicken the shells and reduce the nasal cavity.
The space between the medial wall (septum of the nose) and the nasal conchas, and also between the upper and lower walls forms common nasal passage(meatus nasi communis).In addition, there are separate moves of the nose. Between the lower nasal sink and the lower wall of the nasal cavity lower nasal passage(meatus nasi inferior),between the middle and lower nasal conchas - middle nasal passage(meatus nasi medius),between the upper and middle turbinate - upper nasal passage(meatus nasi superior).Between the upper shell and the front wall of the body of the sphenoid bone lies wedge lattice recess(recessus sphenoethmoidalis),the value of which is different. It opens the sphenoid wedge (Fig. 114).
The width of the nasal passages depends on the size of the cavities, the position of the nasal septum and the state of the mucous membrane.
With disproportionate shells, curvature of the septum and swelling of the mucous membrane, the nasal passages narrow, which can impede nasal breathing. The longest is the lower stroke, the shortest and narrowest - the upper, the widest - the middle.
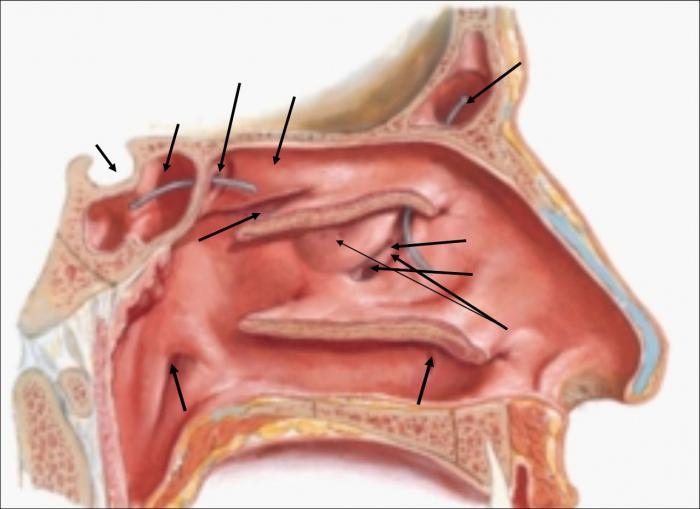
In the lower nasal passage under the arch of the lower shell is a hole lacrimal duct.In the middle nasal passage, the maxillary and frontal sinuses and the front and middle cells of the ethmoid sinus open in separate holes.
On the lateral wall in the area of the middle course is a lunate cleft. (hiatus semilunaris),leading to the frontal sinus, front cells of the ethmoid bone, as well as to the maxillary sinus. Thus, the average nasal passage is clinically an important part of the nasal cavity.
In the upper nasal passage there are openings of the posterior and middle cells of the ethmoid sinus, and in the wedge-ethmoid recess - the aperture of the sphenoid sinus. The rear openings of the nasal cavity - Hoans - are located in its lower part.
The nasal cavity as a whole can be relatively high and short (in brachycephals) or low and long (in dolichocephals). In newborns, the height of the nasal cavity is small. Most often in newborns
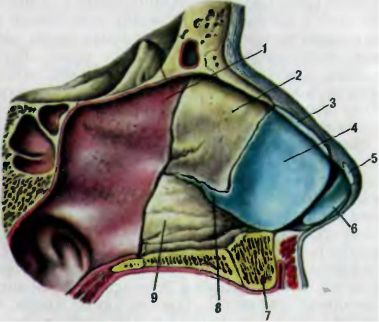
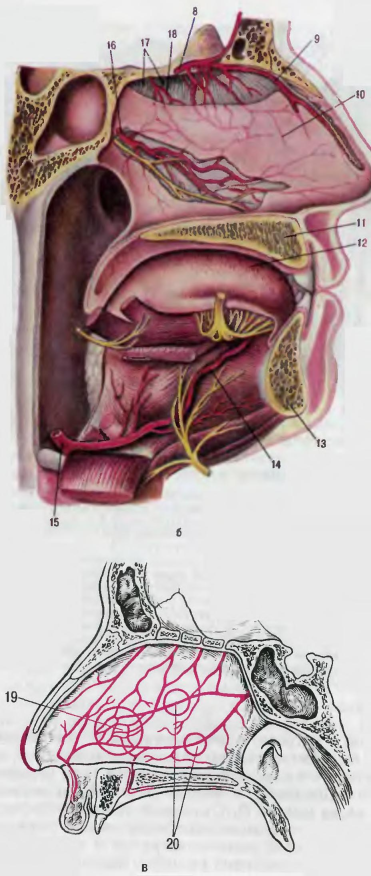
Fig. 114Nose cavity:
a - the lateral wall: 1 - the eve of the nasal cavity; 2 - lower nasal passage; 3 - the threshold of the nose; 4 - lower turbinate; 5 - middle nasal passage; 6 - middle nasal concha; 7 - upper nasal passage; 8 - upper nasal concha; 9 - frontal sinus; 10 - sphenoid sinus; 11 - tube roller; 12 - pharyngeal opening of the auditory tube;
b - the lateral wall after the removal of the turbinates: 1 - the entrance to the maxillary sinus; 2 - opening of the lacrimal duct; 3 - cut off the lower nasal sink; 4 - lunate cleft; 5 - lattice vesicle; 6 - cut off the middle turbinate; 7 - probe in the frontal sinus; 8 - probe inserted through the aperture into the sphenoid sinus;
c - rhinoscopy (examination of the nasal cavity through the nostrils): 1 - median nasal concha; 2 - average nasal passage; 3 - the lower nasal sink; 4 - lower nasal passage; 5 - common nasal passage; 6 - nasal septum
4 sinks: lower, middle, upper and uppermost. The latter is usually subject to reduction and is rare in adults (approximately in 20% of cases). The shells are relatively thick and located close to the bottom and the arch of the cavity, so in infants the lower course of the nose is usually absent and forms only by the 6th-7th month of life. Rarely (in 30% of cases) the upper course of the nose is detected. All 3 nasal passages grow most intensively after 6 months and reach their normal form by the age of 13. Anomalies of size, shape and number of shells are possible.
Mucosa.In the nasal cavity, the mucous membrane is soldered to the underlying periosteum and perichondrium and covered with a multi-row prismatic ciliated epithelium. It contains mucous goblet cells and complex alveolar mucous-serous nasal glands. (gll. nasales).Powerfully developed venous plexuses and arterial networks are located directly under the epithelium, which creates the possibility of warming inhaled air. The most developed cavernous plexus p akovin (plexus cavernosi concharum),damage that causes very heavy bleeding. In the shells, the mucous membrane is especially thick (up to 4 mm). In the olfactory region, the superior nasal concha and partially the vault of the cavity are covered with a special olfactory epithelium.
The mucous membrane of the vestibule of the nose is a continuation of the epithelial lining of the skin and is lined with stratified squamous epithelium. In the connective tissue layer of the vestibule shell laid sebaceous glandsand hair roots.
X-ray anatomy.On radiographs in the anteroposterior and lateral projections are clearly visible nasal septum, its position, shells, paranasal sinuses, as well as changes in anatomical relationships caused by a pathological process or anomalies.
Rhinoscopy.A living person can view the formation of the nasal cavity with a special mirror (rhinoscopy).The cavity mucosa is clearly visible, having pink color in healthy people (in the olfactory region with a yellowish tinge), septum, nasal conchs, passages, some openings of the paranasal sinuses.
Vessels and nerves of the nasal cavity.The blood supply to the nasal cavity is from sphenoid palatine artery(from the maxillary artery). In the front of the blood flows in the branches anterior ethmoid artery(from the ophthalmic artery).
Venous blood flows in 3 directions: into the veins of the cranial cavity - ophthalmic veins, cavernous sinus, anterior section of the upper sagittal
foot sinus; at facial vein;at wedge-palatine vein,flowing into the pterygoid venous plexus.
Lymphatic vessels form from superficial and deep networks and go to pharyngeal, submandibularand chin lymph nodes.
Sensory innervation is provided by the ocular and maxillary nerves (from the V pair of cranial nerves). Autonomic innervation of the glands and vessels of the nasal cavity is provided by sympathetic fibers that go along the vessels of the cavity, and parasympathetic fibers that are suitable as part of the nerves of the pterygo-fibrous node.
Not everyone knows that in the structure of the facial part of the skull there are hollow areas called nasal sinuses. The final formation of this part occurs by 5 years. The sinuses are connected with a special passage to the internal cavity of the nose.
Okolonosovy bosoms, have the different form and the sizes. They may change in the course of various previous diseases. Their inflammation passes with each person in different ways, taking into account individual physiological features.
Anatomy and function of the sinuses
Proper anatomical structure of the nose plays a big role in human health. Internal divisions also include everything. The anatomy of the nasal sinus is no less complicated and important than its functions, so it is worth considering this issue in more detail.
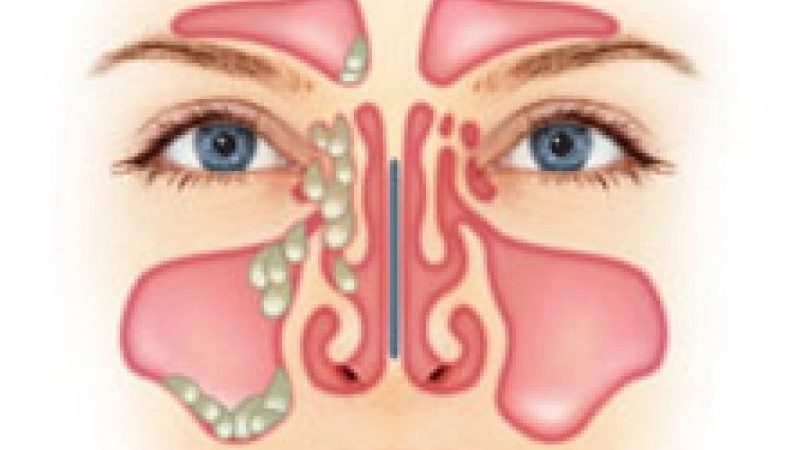
Due to the great importance of the sinuses, it is necessary to react as quickly as possible to the presence of fluid in them.
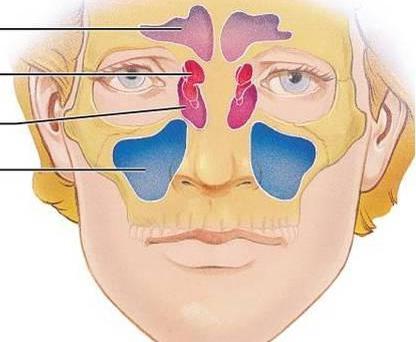
The main sinuses are referred to as wedge-shaped. This name they received due to its location in the sphenoid bone. Due to the fact that they border on other equally important parts of the body (pituitary, carotid arteries, ocular nerves), any inflammation is a great danger.
the biggest of all. They are located in the upper jaw. Each person has a different size. Each has recesses. The structure of the sinuses in its shape resembles a pyramid with three faces.
The inflammatory process in the maxillary sinuses is formed in the fistula. Due to the fact that their lower part borders on the roots of the teeth of the upper jaw, very often any serious dental disease threatens with inflammation.
are in the frontal part above the eyebrows. They are connected to the nasal cavity with an anastomosis. Some people have additional partitions. It is interesting that not all people have frontal (frontal) sinuses, but about 95%. Full size, they reach only at the time of puberty.
Cells of the ethmoid labyrinth. They are located in the ethmoid bone, and their structure resembles interconnected cells that are different in size. Connect to the nasal cavity. The number of such cells reaches 15. The functions of the sinuses completely coincide with the basic functions of the nose.
Conclusion
Despite the fact that the entire system of smell has a rather complicated structure, they are multifunctional and are easily brought back to normal in almost any disease, if you catch it in time and start treatment.
In the event that time does not take up the treatment of diseases, the functioning of this system may be impaired, which would entail problems related to other functions of the body. Therefore, it is necessary to take action on time, together with a specialist.
The nasal cavity (cavum nasi) is located between the oral cavity and the anterior cranial fossa, and from the lateral sides - between the paired upper jaws and paired ethmoid bones. Nasal septum it divides the sagittal into two halves, opening anteriorly with nostrils and posteriorly, in the nasopharynx, by the joans. Each half of the nose is surrounded by four pneumatic paranasal sinuses: the maxillary, ethmoid labyrinth, frontal and sphenoid, which communicate on its side with the nasal cavity (Fig. 1.2). The nasal cavity has four walls: lower, upper, medial and lateral; posterior nasal cavity through Joan communicates with the nasopharynx, the front remains open and communicates with the outside air through the holes (nostrils).
1-upper nasal passage; 2 - sphenoid sinus; 3 - superior nasal concha; 4 - pharyngeal mouth of the auditory tube; 5 - middle nasal passage; 6 - additional fistula of the maxillary sinus; 7 - hard sky; 8 - the lower nasal sink; 9 - lower nasal passage; 10 - the eve of the nose, 11 - the middle nasal conch, 12 - the frontal sinus and the bellied probe inserted into its lumen through the frontal-nasal canal.
The lower wall (the bottom of the nasal cavity) is formed by two palatal processes of the upper jaw and, in a small area of the posterior part, by two horizontal plates of the palatine bone (hard palate). By a similar line, these bones are connected by a suture. Violations of this compound lead to various defects (cleft of the palate, cleft lip). In the front and in the middle in the bottom of the nasal cavity there is a nasal channel (canalis incisivus), through which the same-name nerve and artery anastomosing in the canal with the large palatine artery pass into the oral cavity. This circumstance must be kept in mind when performing submucous resection of the nasal septum and other operations in this area in order to avoid significant bleeding. In newborns, the bottom of the nasal cavity is in contact with the tooth buds, which are located in the body of the upper jaw.
The upper wall (roof) of the nasal cavity is formed in the front by the nasal bones, in the middle sections by the ethmoid plate (lamina cribrosa) and the ethmoid cells (the largest part of the roof), the back sections are formed by the front wall of the sphenoid sinus. Threads of the olfactory nerve pass through the holes in the ethmoid plate; the bulb of this nerve lies on the cranial surface of the ethmoid plate.
It must be borne in mind that in the newborn lamina cribrosa is a fibrous formation that ossifies only by 3 years.
The medial wall, or nasal septum (septum nasi), consists of the anterior cartilaginous and posterior bone sections (Fig. 1.3). The bone section is formed by the perpendicular plate (lamina perpendicularis) of the ethmoid bone and vomer (vomer), the cartilaginous - quadrangular cartilage, the upper edge of which forms the anterior part of the back of the nose. On the eve of the nose, anteriorly and downwards from the front edge of the quadrangular cartilage, there is an outside skin-webbed mobile part of the nasal septum (septum mobile). In a newborn, the perpendicular plate of the ethmoid bone is represented by a membranous formation, the ossification of which ends only by 6 years. The nasal septum is usually not exactly in the median plane. Significant curvatures of her in the anterior section, more common in men, can cause disturbances in breathing through the nose. It should be noted that in a newborn the height of the opener is less than the width of the choana, therefore it appears as a transverse slit; only by the age of 14, the height of the opener becomes greater than the width of the choana, and it takes the form of an oval that extends upwards.
1 - the mucous membrane of the nasal cavity; 2 - perpendicular plate of the ethmoid bone; 3 - triangular lateral cartilage; 4 - quadrangular cartilage of the nasal septum; 5 - small cartilage of the wing of the nose; 6 - the medial leg of the large cartilage of the wing of the nose; 7 - nasal crest; 8 - wedge-shaped process of the cartilage of the nasal septum; 9 - coulter
The structure of the lateral (outer) cavity wall is more complicated (Fig. 1.4). In its formation take part in the front and middle parts medial wall and frontalis of the upper jaw, lacrimal and nasal bones, the medial surface of the ethmoid bone, in the posterior part, forming the edges of the choanal, is the perpendicular process of the palatine bone and the prilar processes of the sphenoid bone. On the outer (lateral) wall are three turbinates (conchae nasales): the lower (concha inferior), the middle (concha media) and the upper (concha superior). The lower shell is an independent bone, the line of its attachment forms an arc, convex upwards, which should be considered when puncturing the maxillary sinus and conchotomy. The middle and upper shells are processes of the ethmoid bone. Often the front end of the middle shell is inflated in the form of a bubble (conhae bullosa) - this is an air-cell of the ethmoid labyrinth. Anterior to the middle shell there is a vertical bone protrusion (agger nasi), which can be expressed to a greater or lesser extent. All the nasal conchs, attaching with one lateral edge to the lateral wall of the nose in the form of elongated flattened formations, with the other edge hang downwards and medially in such a way that the lower, middle and upper nasal passages are formed respectively, the height of which is 2-3 mm. A small space between the top of the sink and the roof of the nose, called sphenoemoidal,

A - with preserved relief structure: 1 - sphenoid sinus; 2 - additional cell of the sphenoid sinus; 3 - upper nasal concha; 4 - upper nasal passage, 5 - median nasal concha; 6 - pharyngeal mouth of the auditory tube; 7 - nasopharynx; eight - uvula; 9 - language; 10 - hard sky; 11 - the lower nasal passage; 12 - the lower nasal sink; 13 - additional fistula of the maxillary sinus; 14 - hooked process; 15 - semilunar gap; 16-lattice bulla; 17-pocket lattice bulla; 18 - frontal sinus; 19 - cells of the ethmoid labyrinth.

B - with open sinuses: 20 - lacrimal sac; 21 pockets of the maxillary sinus; 22 - nasolacrimal canal; 23 - a back cage of a trellised labyrinth; 24 - front cells of the ethmoid labyrinth; 25 - the fronto-nasal canal.
Usually referred to as the upper nasal passage. Between the nasal septum and the nasal concha remains a free space in the form of a slit (3-4 mm in size), which extends from the bottom to the roof of the nose - a common nasal passage.
In a newborn, the lower conch descends to the bottom of the nose, the relative narrowness of all nasal passages is noted, which causes a rapid onset of difficulty in nasal breathing in young children, even with a slight swelling of the mucous membrane due to its catarrhal state.
On the side wall of the inferior nasal passage at a distance of 1 cm in children and 1.5 cm in adults from the anterior end of the shell is the nasolacrimal duct. This hole is formed after birth; in case of delaying it from opening, the outflow of tear fluid is disturbed, which leads to cystic dilation of the canal and narrowing of the nasal passages.
The bone of the lateral wall of the lower nasal passage at the base is much thicker than that of the line of attachment of the lower shell (this must be borne in mind when puncturing the maxillary sinus). The posterior ends of the lower cavities closely fit the pharyngeal orifices of the auditory (Eustachian) tubes on the lateral walls of the pharynx, as a result of which the hypertrophy of the shells may impair function. auditory tubes and develop their disease.
The middle nasal passage is located between the lower and middle shells, on its lateral wall there is a crescent-shaped (semi-lunar) slit (hiatus semilunaris), the back section of which is located below the front (first described by N.I. Pirogov). In this slot open: in the back section - maxillary sinus through the hole (ostium1maxillare), in the anterior-upper section - the opening of the canal of the frontal sinus, which does not form a straight line, which must be borne in mind when probing the frontal sinus. The crescent-shaped gap in the posterior part is limited by the protrusion of the ethmoidal labyrinth (bulla ethmoidalis), and in the anterior region by the hooked process (processus uncinatus), which departs anterior to the anterior edge of the middle turbinate. The medial nasal passage also opens the anterior and middle cells of the ethmoid bone.
The upper nasal passage extends from the middle shell to the roof of the nose and includes sphenoemoidal space. At the level of the posterior end of the upper shell, the sphenoid sinus is opened through the opening (ostium sphenoidale) into the upper nasal passage. The posterior cells of the ethmoid labyrinth also communicate with the superior nasal passage.
The mucous membrane of the nasal cavity covers all its walls with a continuous layer and continues into the paranasal sinuses, pharynx and middle ear; it has no submucosal layer, which is absent in the respiratory tract at all, with the exception of the subglossal region of the larynx. The nasal cavity can be divided into two sections: the anterior - the vestibule (vestibulum nasi) and the actual nasal cavity (cavum nasi). The latter, in turn, is divided into two areas: respiratory and olfactory.
Regio respiratoria (regio respiratoria) occupies the space from the bottom of the nose up to the level of the lower edge of the middle shell. In this area, the mucous membrane is covered with a multi-row cylindrical ciliary epithelium.
Under the epithelium is the actual tissue of the mucous membrane (tunica propria), consisting of connective tissue collagen and elastic fibers. There is a large number of goblet cells that produce mucus, and the trumpeted-alveolar branched glands, producing a serous or serous-mucous secretion, which through the excretory ducts exits onto the surface of the mucous membrane. Slightly below these cells, basal cells are located on the basement membrane, which are not subject to desquamation. They are the basis for the regeneration of the epithelium after its physiological and pathological desquamation (Fig. 1.5).
The mucous membrane is tightly soldered all the way to the perchondrium or periosteum, which makes up a single whole with it, therefore during the operation the membrane is separated with these formations. In the region of the predominantly medial and lower parts of the lower shell, the free edge of the middle shell and their posterior ends, the mucous membrane is thickened due to the presence of cavernous tissue consisting of dilated venous vessels whose walls are richly supplied with smooth muscles and connective tissue fibers. Portions of the cavernous tissue can sometimes be found on the nasal septum, especially in its posterior part. Filling and emptying the cavernous tissue with blood occurs reflexively under the influence of various physical, chemical and psychogenic stimuli. Mucous membrane containing cavernous tissue
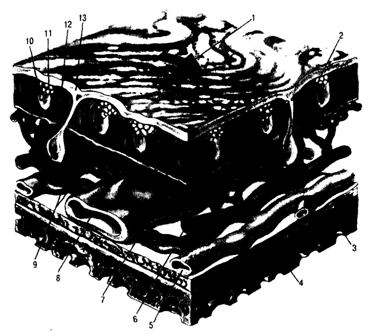
1-direction of mucociliary flow; 2 - mucous gland; 3 - the periosteum; 4 - bone; 5-vein; 6th artery; 7 - arteriovenous shunt; 8 - venous sinus; 9 - submucous capillaries; 10 - goblet cell; II - hair cell; 12 - the liquid component of mucus; 13 - viscous (gel) component of mucus.
It can instantly swell (thereby increasing the surface and warming the air to a greater extent), causing a narrowing of the nasal passages, or shrinking, having a regulating effect on the respiratory function. In children, the cavernous venous formations reach their full development by the age of six. At a younger age, rudiments of the Jacobson olfactory organ are sometimes found in the mucous membrane of the nasal septum, located at a distance of 2 cm from the front edge of the septum and 1.5 cm from the bottom of the nose. Here cysts can form and develop inflammatory processes.
Regina olfactoria (regio olfactoria) is located in its upper sections, from the arch to the lower edge of the middle turbinate. In this area, the mucous membrane is covered by the olfactory epithelium, the total area of which in one half of the nose is about 24 cm2. Among the olfactory epithelium in the form of islets, there is a ciliated epithelium, which performs a cleaning function here. The olfactory epithelium is represented by olfactory fusiform, basal and supporting cells. The central fibers of the spindle-shaped (specific) cells pass directly into the nerve fiber (fila olfactoria); the tops of these cells have protrusions into the nasal cavity - olfactory hairs. Thus, the spindle-shaped olfactory nerve cell is both a receptor and a conductor. The surface of the olfactory epithelium is covered with the secret of specific tubular-alveolar olfactory (bowman) glands, which is a universal solvent of organic substances.
The nasal cavity (Fig. 1.6, a) is provided with the terminal branch of the internal carotid artery (a.ophthalmica), which gives the lattice arteries in the orbit (aa.ethmoidales anterior et posterior); these arteries feed the anteroposterior sections of the walls of the nasal cavity and the ethmoid labyrinth. The largest artery of the nasal cavity is a.sphe-nopalatina (a branch of the internal maxillary artery from the system of the external carotid artery), it leaves the pterygopalatine fossa through the opening formed by the processes of the vertical plate of the palatal bone and the body of the main bone (foramen sphenopalatinum) (Fig. 1.6, b ), gives the nasal branches to the side wall of the nasal cavity, septum and all the paranasal sinuses. This artery is projected on the side of the nose near the posterior ends of the middle and lower turbinates, which must be borne in mind when performing operations in this area. A special feature of the vascular septum is the formation of a thick vascular network in the mucous membrane in the region of its anterior third (locus Kisselbachii), here the mucous membrane is often thinned (Fig. 1.6, c). Nasal bleeding occurs more often from this place than from other areas, so it is called the "bleeding area of the nose." Venous vessels accompany the arteries.
A feature of the venous outflow from the nasal cavity is its connection with the venous plexuses (plexus pterigoideus, sinus cavernosus), through which the nasal veins communicate with the veins of the skull, orbit and pharynx, as a result of which it is possible to spread the infection along these routes and the occurrence of rhinogenic intracranial and orbital complications, sepsis and others
L and m f about about t about about from the anterior sections of the nose is carried out in the submandibular the lymph nodes, from the middle and posterior parts - into the deep cervical. It is important to note the connection lymphatic system olfactory region of the nose with b-annular spaces, carried out along the perineural pathways of the olfactory nerve fibers. This explains the possibility of meningitis after an operation on the lattice labyrinth.
And - a lateral wall of a nasal cavity: 1 - posterolateral nasal arteries; 2 - anterolateral nasal artery; 3-nasal disease artery; 4 - large palatine artery; 5 - ascending palatine artery; 6 - small palatine artery; 7 - palatine artery; b - the medial wall of the nasal cavity: 8 - the anterior ethmoid artery; 9 - the anterior artery of the nasal septum; 10 - mucous membrane of the nasal septum; 11 - the upper jaw; 12 - language; 13 - lower jaw; 14 - deep artery of the tongue; 15 lingual artery; 16 - posterior artery of the nasal septum; 17 - holed (sieve) plate of the ethmoid bone; 18 - posterior ethmoid artery; c - blood supply to the nasal septum 19 - Kisselbach zone; 20 - a dense network of anastomoses of the arteries of the nasal septum and the system of the internal main palatine artery.
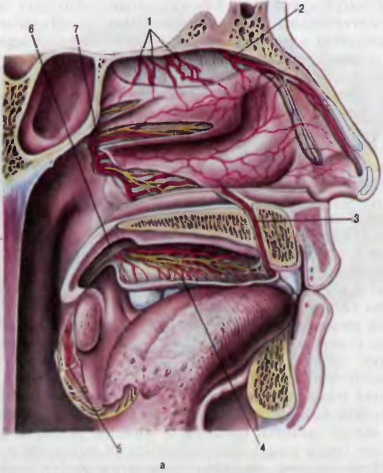
In the nasal cavity, olfactory, sensitive and secretory are distinguished. Olfactory fibers (fila olfactoria) diverge from the olfactory epithelium and through the ethmoid plate penetrate the cranial cavity to the olfactory bulb, where they form synapses with the dendrite of the olfactory tract cells (olfactory nerve). The parahippocampal gyrus (gyrus hippocampi), or seahorse gyrus, is the primary center of smell, the hippo-bark
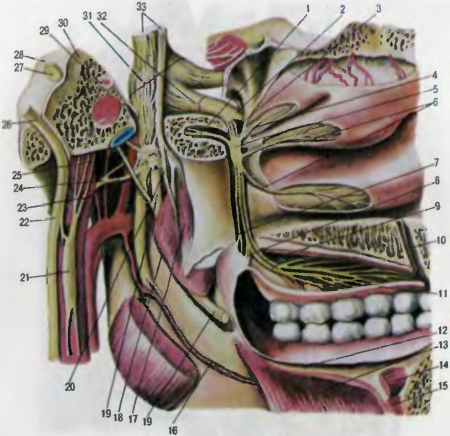
1 - pterygoid nerve nerve; 2 - infraorbital nerve; 3 - the main palatine nerve; 4 - posterolateral nasal branches; 5 - basic palatal node; 6 - posterolateral nasal branches; 7-back palatine nepv, 8 middle palatine nerve; 9 - anterior palatine nerves; 10 - nasal nerve; 11 - nasal mucosa; 12 - oral mucosa; 13 - maxillary-hypoglossal muscle; 14 - chin-tongue muscle; 15 - chin-hypoglossal muscle; 16 - maxillary hypoglossal nerve; 17 - muscle tipping the palatine curtain; 18 - internal pterygoid muscle; 19 - lingual nerve; 20 - internal pterygoid nerve; 21 - superior cervical ganglion; 22 - the ganglion of the vagus nerve: 23 - the temporal arch. 24 - ear node; 25 - drum string; 26 - jugular node of the vagus nerve; 27 - VIII pair of cranial nerves (pre-door-cochlear nerve); 28 - facial nerve; 29 - large surface stony nerve; 30 - mandibular nerve; 31 - semilunar node; 32 - maxillary nerve; 33 - trigeminal nerve (large and small portions).
The Kampa (ammonium horns) and the anterior perforative substance are the highest cortical center of smell.
Sensitive innervation of the nasal cavity is carried out by the first (n.ophtalmicus) and second (n.maxillaris) branches trigeminal nerve (Fig. 1.7). From the first branch of the trigeminal nerve, the anterior and posterior ethmoid nerves leave, which penetrate into the nasal cavity along with the vessels and innervate the lateral divisions and the nasal vault. to the septum of the nose. The infraorbital nerve departs from the second branch to the mucous membrane of the bottom of the nasal cavity and maxillary sinus. The branches of the trigeminal nerve anastomose among themselves, which explains the irradiation of pain from the nose and paranasal sinuses to the teeth, eyes, dura (pain in the forehead, occiput), etc. The sympathetic and parasympathetic innervation of the nose and paranasal sinuses is represented by the nerve of the pterygopathic canal (vidia nerve), which originates from the plexus on the internal carotid artery (upper cervical sympathetic node) and the articular nodular nerve (parasympathetic portion).
The nasal cavity is the beginning of the airway. It is through her that the air enters the body through a special channel that connects the external environment and the nasopharynx. In addition to the main respiratory function, it performs a number of tasks: protection, cleansing and moisturizing. With age, the size of the cavity increases, in the elderly it is about three times larger than in infants.
Structure
The nasal cavity is a rather complicated formation. It consists of several parts, which directly include the outer part of the nose and the nasal passage, the row of bones of the skull with which it is formed, the cartilage covered with the outside skin, and from the inside - mucous membrane. This is just a general list of what the nasal cavity consists of.
Its structure is rather complicated. So, the outer part of the nose is the wings (or the more popular name is the nostrils) and the back. The last part includes the middle part and the root, which goes to the frontal part of the face. From the side oral cavity nose is limited to hard and soft palate. And inside the cavity is formed by the bones of the skull.
The nose itself consists of two nostrils, between which a cartilaginous septum is installed. Each of them has posterior, lower, lateral, upper and medial walls. Also, the anatomy of the nose includes a special area that consists of blood vessels. By the way, this is one of the causes of frequent bleeding in this area. The septum divides the nose into 2 parts, but not all of them are the same. It can be curved as a result of damage, injury, or due to the appearance of formations.
Nasal passages are conventionally divided into the vestibule and the cavity itself. The first part is lined with squamous epithelium and covered with small hairs. And directly in the nasal cavity is the ciliated epithelium.
Outside travel
 Do not forget that the purification of the air is still in the nostrils. At the entrance there are bunches of hair that are designed to hold large particles of dust coming from the air. And the inner surface of the passage is lined with mucous glands that protect the body from the incoming microbes, reducing their ability to reproduce.
Do not forget that the purification of the air is still in the nostrils. At the entrance there are bunches of hair that are designed to hold large particles of dust coming from the air. And the inner surface of the passage is lined with mucous glands that protect the body from the incoming microbes, reducing their ability to reproduce.
The nose has a root, which is located between the sockets. His back is facing down. The lower part of the nose, where the air intakes are located, the nostrils, is called the apex. By the way, the holes through which breathing is carried out, for all people of different sizes. This is due to the fact that the septum unevenly divides the nose, it passes not strictly in the middle, but is rejected in some direction.
The wings of the nose are located on the lateral sides. The outer part of it is formed by two bones and cartilage. The latter are located in the septum of the nose and, with their lower edge, are connected to the soft tissues located there. In the wings of the nose is also up to 4 cartilaginous elastic plates, between them is the connective tissue, and they are covered with facial muscles.
Cavities
The structure also includes the paranasal sinuses: wedge-shaped, frontal, maxillary, cells of the ethmoid labyrinth. They are divided into front and rear. This classification is necessary primarily for doctors, because their pathologies are different.
Paired maxillary sinuses The nasal cavity is also called the maxillary. In shape, they resemble a pyramid. They received the second name due to their location. One wall they border the nasal cavity. It has a hole that connects the sinus with the middle nasal passage, it is its overlap that leads to the development of inflammation, which is called sinusitis. On top of the cavity is limited to the lower wall of the orbit, and its bottom reaches the roots of the teeth. For some, they may even pass into this sinus. Therefore, sometimes even ordinary caries causes odontogenic sinusitis.
The size of the maxillary cavities may vary, but each of them has additional indentations. They are called coves. Experts distinguish zygomatic, palatal, frontal, alveolar depressions.
The nasal cavity of a person includes the paired frontal sinuses. Their back walls border the brain, its frontal lobes. In their lower part there is a hole that connects them with the fronto-nasal canal leading to the middle nasal passage. With the development of inflammation in this area establish the diagnosis of frontal sinusitis.
In the sphenoid bone is the same sinus. Its upper wall rests against the pituitary gland, the lateral wall of the cranial cavity and the carotid artery, the lower one goes to the nose and nasopharynx. Because of this neighborhood, inflammation in this area is considered dangerous, but, fortunately, it is quite rare.
Also otolaryngologists distinguish the ethmoid sinuses. They are located in the nasal cavity and are divided into posterior, middle and anterior depending on the place of their dislocation. The front and middle connect with the middle nasal passage, and the rear - with the top. In essence, this is a union of cells of the ethmoid bone of various sizes. They are connected not only with the nasal cavity, but also among themselves. Each person can have from 5 to 15 of the specified sinuses, which are located in 3 or 4 rows.
Structure formation
In the process of human growth, starting from his birth, the nasal cavity changes. For example, children have only two sinuses: the ethmoid labyrinth and the maxillary. At the same time in infants can be found only their beginnings. They develop in the process of growth. The frontal cavities of babies are absent. But in about 5% of people they do not appear over time.
Also, children have significantly narrowed nasal passages. This often becomes the cause of difficulty breathing crumbs. The back of the root of the nose in newborns is not particularly pronounced. Their final formation is completed only by 15 years.
Do not forget that with age they begin to die nerve endings - neurons responsible for the sense of smell. That is why older people often do not hear many smells.
Breathing
 In order for the air not only to enter the body, but also to be cleaned, it is provided for humidification so that the nasal cavity has a specific shape. Its structure and functions provide a special passage of air.
In order for the air not only to enter the body, but also to be cleaned, it is provided for humidification so that the nasal cavity has a specific shape. Its structure and functions provide a special passage of air.
The cavity consists of three shells, which are separated by passages. It is on them that the air flows. It is worth noting that only the lower shell is true, because, unlike the middle and upper shell, it is formed by bone tissue.
The lower course is connected to the orbit through the nasal duct. The median is associated with maxillary and frontal sinuses, it forms the middle and front cells of the trellised labyrinth. The posterior end of the superior nasal concha forms the sinus of the main bone. The upstroke is the posterior cells of the ethmoid bone.
The sinuses are accessory cavities of the nose. They are expelled by a membrane containing a small amount of mucous glands. All partitions, shells, sinuses, accessory cavities significantly increase the surface of the walls belonging to the upper airway. Thanks to all the plexus, the nasal cavity is formed. Its structure is not limited to internal labyrinths. It includes the outer part, designed for air intake, its purification, heating.
The principle of the upper respiratory tract

When entering the external nasal passage, air enters a well-heated cavity. Heat it is achieved due to the large number of blood vessels. The air warms up quickly enough and reaches body temperature. At the same time in the same place it is cleared of dust and microbes due to the natural barrier of tufts of hair and mucus. Also, in the upper part of the nasal cavity, the olfactory nerve branches. It controls the chemical composition of the air and regulates the force of inhalation depending on it.
When the nasal cavity ends, the structure and functions of which are designed to provide breathing, the nasopharynx begins. It is located behind the nasal and oral cavity. Its lower part is divided into 2 tubes. One of them is respiratory, and the second is the esophagus. They cross in the throat. This is necessary so that a person can breathe air in an alternative way - through the mouth. This method is not very convenient, but it is necessary in cases where the nasal passages are closed. After all, it is for this purpose that the oral and nasal cavities are connected, they are separated only by the palatal wall.
But it is worth noting that when breathing through the mouth, the air is not able to properly clean and warm up. That is why healthy people should always try to breathe air solely with their nose.
Mucosa
Starting from the outer part of the nose, the inner surface of the cavity is lined with special cells. On each cm 2 there are about 150 mucous glands. They produce substances that have a protective function. The nasal mucosa is designed to protect the body from the harmful effects of germs that enter it through the air. Their main action is aimed at reducing the ability of pathological organisms to reproduce. But besides this, through the cellular cracks of the blood vessels, a large number of leukocytes are released into the cavity. They counteract the incoming microbial flora.
A huge part of the nasal cavity and its sinuses, covered with small filiform cilia. Several dozen such formations depart from each cell. They constantly hesitate, making wavy movements. They quickly bend toward the holes to exit, and slowly return in the opposite direction. If you greatly increase them, you get a picture that resembles a field of wheat, which is excited by the force of the wind.
In the nasal cavity air must be cleaned. And the ciliary epithelium serves precisely so that the detained microparticles can be rapidly removed from the nasal cavity.
Cavity function
In addition to providing breathing, the nose is designed to perform a number of other tasks. Scientists have found that proper breathing ensures the correct functioning of the whole organism. So, the main functions of the nasal cavity:
1) Breathing: it is thanks to the flow of air from the external environment that all tissues are saturated with oxygen;
2) protection: during the passage through the nose, the air is purified, warmed, disinfected;
3) sense of smell: recognition of odors is necessary not only in a number of professions (for example, in the food, perfume or chemical industry), but also for normal life activity.
The reflex challenge of necessary actions can also be attributed to the protective function: it can be sneezing or even a temporary stop of breathing. The necessary signal is sent to the brain by nerve endings when irritant substances get on them.

Also, it is the nasal cavity that performs the resonator function - it gives voice to sonority, tonality and individual color. Therefore, when the head cold, it changes, becomes nasal. By the way, it is full nasal breathing that stimulates normal blood circulation. It contributes to the fact that there is a normal outflow of venous blood from the skull, improves lymph circulation.
Do not forget that the nose and nasal cavity have a special structure. It is because of the large number of airway sinuses significantly facilitated mass of the skull.
Providing a protective function
Many tend to underestimate the importance of nasal breathing. But without the normal execution of this function, the body is more susceptible to infections. The entire inner surface of the nose should be slightly moistened. This is due to the fact that the goblet cells and the corresponding glands produce mucus. All particles that fall into the nose are glued to it and removed with the help of ciliary epithelium. The process of cleansing depends on the state of this layer, which provides the basic functions of the nasal cavity. If the cilia are damaged, and this can occur as a result of the illness or injury, the movement of mucus will be disturbed.
Also to protect serve lymphatic follicles, which are located on the eve of the nasal cavity and perform immunomodulatory function. Plasma cells, lymphocytes and occasionally occasional granular leukocytes are intended for the same. All of them are the gateway to pathogenic bacteria that can enter the body with air.
Possible problems
In some cases, the nasal cavity can not perform all its functions in full. If problems arise, breathing becomes difficult, the protective function weakens, the voice changes, the sense of smell is temporarily lost.
 The most common disease is rhinitis. It can be a vasomotor - at the heart of the problem is treating the deterioration of the tone of the vessels that are in the submucosa of the lower shells. Allergic rhinitis - this is just an individual reaction of the body to potential stimuli. These include dust, fluff, pollen and others. Hypertrophic rhinitis is characterized by an increase in connective tissue. It develops as a consequence of other species. chronic diseases the nose. Also, a runny nose may be due to taking too long. vasoconstrictor drugs. This phenomenon is called medical rhinitis.
The most common disease is rhinitis. It can be a vasomotor - at the heart of the problem is treating the deterioration of the tone of the vessels that are in the submucosa of the lower shells. Allergic rhinitis - this is just an individual reaction of the body to potential stimuli. These include dust, fluff, pollen and others. Hypertrophic rhinitis is characterized by an increase in connective tissue. It develops as a consequence of other species. chronic diseases the nose. Also, a runny nose may be due to taking too long. vasoconstrictor drugs. This phenomenon is called medical rhinitis.
The mucous membrane of the nasal cavity may suffer due to injury or surgery. In these cases, synechiae may occur. Also in cases of advanced rhinosinusitis, excessive mucosal growth is observed. In many situations, this is accompanied by allergic rhinitis. Another problem the patient may face is the appearance of tumors. There may be cysts, osteomas, fibroids or papillomas in the nose.
Also, do not forget that it is often not the nasal cavity itself that suffers, but the paranasal sinuses. Depending on the site of inflammation, the following diseases are distinguished.
- With the defeat of the maxillary sinuses develops sinusitis.
- Inflammatory processes in areas of the ethmoid labyrinth are called ethmoiditis.
- Frontal disease is called pathological problems with the frontal cavities.
- In cases when it comes to inflammation of the main sinus, they talk about sphenoiditis.
But it happens that problems begin in all cavities at the same time. Then the otolaryngologist can make a diagnosis of pansinusitis.
ENT doctors can diagnose the acute or chronic nature of the disease. They are distinguished by the degree of symptoms and the frequency of manifestations of the disease. Often to problems with sinuses cause common colds that were not cured in time.
Most often, experts are faced with sinusitis or frontal. This is due to the structure and location of the frontal and maxillary sinuses. It is because of this that they are most often affected. Feeling painful sensations in the area of these cavities, it is better to go to the otolaryngologist, who will be able to diagnose and select an adequate treatment.
Outside, the nose consists of wings, or nostrils, the back of the middle part and the root located in the frontal lobe of the face. Inside its walls are formed by the bones of the skull, and from the side of the mouth it is limited to a hard and soft palate. It has a complex structure - the nasal cavity is divided into two nostrils, each of which has a medial (septum between the nostrils), lateral, upper, lower and back walls.
In addition to bone tissue, the membranous and cartilaginous components of high mobility are included in the structure of the nasal cavity. There are three sinks in the cavity.- upper, middle and lower, but only the last true, since it is alone formed by an independent bone. The passages are located between the shells - the spaces through which the air flows:
upper turn. It is located at the back and has openings in the cell of the ethmoid bone;
middle move It communicates with its frontal cells, with the frontal and maxillary sinuses;
lower turn. It connects through the nasal duct with the orbit.
The nasal cavity consists of the vestibule and the respiratory part.
The vestibule of the nose is lined with mucous membrane, which is composed of a multi-layered flat non-squaring epithelium and its own mucous plate.
The respiratory part is lined with a single layer of multi-row ciliary epithelium. In its composition are distinguished:
ciliated cells - have ciliated cilia that oscillate against the movement of inhaled air, with the help of these cilia microorganisms are removed from the nasal cavity and foreign bodies;
goblet cells secrete mucins - mucus, which sticks together foreign bodies, bacteria and facilitates their excretion;
microvillous cells are chemoreceptor cells;
basal cells play the role of cambial elements.
The lamina propria of the mucosa is formed by loose, fibrous, unformed connective tissue, and simple tubular protein-mucous glands, vessels, nerves and nerve endings, as well as lymphoid follicles, lie in it.
The mucous membrane lining the respiratory part of the nasal cavity has two areas that differ in structure from the rest of the mucosa:
the olfactory part, which is located on the greater part of the roof of each nasal cavity, as well as in the upper turbinate and the upper third of the nasal septum. The mucous membrane lining the olfactory region forms the olfactory organ;
the mucous membrane in the region of the middle and lower turbinates differs from the rest of the nasal mucosa in that it contains thin-walled veins resembling the lacunae of the cavernous bodies of the penis. Under normal conditions, the blood content in the gaps is small, since they are in a partially collapsed state. With inflammation (rhinitis), the veins overflow with blood and constrict the nasal passages, making it difficult for nasal breathing.
The olfactory organ is the peripheral part of the olfactory analyzer. The composition of the olfactory epithelium includes three types of cells:
olfactory cells have a spindle shape and two processes. The peripheral process has a thickening (olfactory mace) with antennas - olfactory cilia that run parallel to the surface of the epithelium and are in constant motion. In these processes, upon contact with an odorous substance, a nerve impulse is formed, which is transmitted along the central process to other neurons and further to the cortex. Olfactory cells are the only type of neurons that have a precursor in the form of cambial cells in an adult individual. Thanks to the division and differentiation of basal cells, olfactory cells are updated every month;
supporting cells are located in the form of a multi-row epithelial layer, on the apical surface have numerous microvilli;
basal cells have a conical shape and lie on the basement membrane at some distance from each other. Basal cells are undifferentiated and serve as a source for the formation of new olfactory and supporting cells.
Axons of olfactory cells, vascular venous plexus, as well as secretory sections of simple olfactory glands are located in the lamina propria of the olfactory region. These glands produce protein secretion and secrete it to the surface of the olfactory epithelium. The secret dissolves odorous substances.
The olfactory analyzer is built from 3 neurons.
The first neuron is the olfactory cells, their axons form the olfactory nerves and end in the form of glomeruli in the olfactory bulbs on the dendrites of the so-called mitral cells. This is the second link of the olfactory path. The axons of mitral cells form olfactory pathways in the brain. The third neurons are cells of the olfactory tracts, the processes of which end in the limbic region of the cerebral cortex.
The nasopharynx is a continuation of the respiratory part of the nasal cavity and has a structure similar to it: it is lined with a multi-row ciliated epithelium lying on its own lamina. The secretory sections of the small protein-mucous glands lie in the lamina propria, and the lymphoid tissue (pharyngeal tonsil) is located on the back surface of the lymphoid tissue.
The structure of the paranasal sinuses.
The near-nasal sinuses consist of several parts that are interconnected.
The maxillary sinus is the air-cavity, adjacent to the nasal cavity and communicating with it by the maxillary orifice, which opens in the middle nasal passage. The near-nasal sinuses, to which the maxillary sinus belongs, also appear in the form of primordia in the embryonic period of fetal development; changing their shape and size, they continue to develop in the postnatal period and are finally formed at the age of 14–20 years.
Maxillary sinus- the largest paranasal sinus. It is located in the thickness of the upper jaw and in form resembles a trihedral pyramid, the base of which is the external wall of the nasal cavity, and the tip is the zygomatic process of the upper jaw. The capacity of the sinus varies between 3-30 cm cubic, averaging 10-12 cm cubic. The air pressure in it is normally the same as in the nasal cavity.
The variability of the volume of the sinus due to the conditions of its development.
It was found that the maxillary sinus is formed due to resorption of the spongy substance of the upper jaw. It is possible that the chewing apparatus function influences this process. In cases where resorption occurs slowly and rather ends, the size of the maxillary sinus are so small that it can be taken as rudimentary; the walls of such a sinus are thick. Good bone resorption leads to the formation of a large sinus. According to German doctors, the narrowing of the maxillary sinus can also occur as a result of: 1) the convergence of the outer and inner walls of the sinus between themselves; 2) strong protrusion of the nasal wall and in the direction of the maxillary sinus; 3) thickening of the walls of the maxillary sinus; 4) tooth retention in the alveolar process; 5) combinations of all these conditions.
The inner wall of the maxillary sinus is the outer wall of the nasal cavity. This wall is the most difficult in the anatomical respect and has important clinical significance. It includes the nasal bones, the medial surface of the body of the upper jaw with the frontal process, the lacrimal bone, the cells of the ethmoid labyrinth, the perpendicular plate of the palatine bone and the inner plate of the pterygoid process of the main bone.
The inner wall of the maxillary sinus is mainly projected on the lower and middle nasal passages. Bone wall gradually thinning from the bottom up and from front to back and in the central part of the middle nasal passage is completely absent. Here the wall consists of a duplicature of the mucous membrane.
On the inner wall of the maxillary sinus at the base of the orbit there is a hole through which the maxillary sinus communicates with the nasal cavity in the area of the anterior section of the middle nasal passage.
The size of the hole is 2-19 mm in length and 2-6 mm in width. The hole located on the wall of the sinus does not correspond strictly to the mouth of the sinus in the nasal cavity and can be removed from it at a distance of 1 cm, resulting in an oblique canal. This circumstance in combination with the high position of the hole makes it difficult to outflow from the sinus. In some cases (10%) posterior to the first, main hole, there is a second, auxiliary, hole.
Through the maxillary hole air is exchanged in the sinus. Doctors have determined that with a normally functioning opening, the air in the cavity is exchanged by 90% for 5 minutes. The permeability of the maxillary opening is of great importance in the development of pathological processes in the sinuses.
The inner wall in the upper-posterior section is in close contact with the cells of the ethmoid labyrinth, which in some cases bulge into the sinus.
The upper wall of the maxillary sinus is the lower wall of the orbit. This is a thin bone plate, in which there are sometimes degiscension, covered with mucous membrane. In the thickness of this plate is the infraorbital canal, in which the same nerve, artery and vein pass. The channel in the form of a roller is contoured on the lower, sinus surface of the plate. Inogra in the specified cushion there are crevices and then the nerve and vessels passing in the canal are covered only with a thin mucous membrane, which should be considered when scraping the upper wall during sinus surgery.
The front, or facial, wall is the thickest, covered with soft cheek tissues and palpation is available. In the center of the front wall there is a groove - the canine fossa, which serves as a guide when opening the mandibular sinus. In this place the bone is the thinnest. At the upper edge of the canine fossa there is a hole through which the second branch of the trigeminal nerve, the infraorbital nerve, comes to the surface. The back wall is bordered by the infratemporal and pterygo-pits, in the latter the pterygoid venous plexus is located.
The lower wall of the maxillary sinus is the posterior part of the alveolar process of the upper jaw. The bottom wall is in close contact with the holes of the first, second large molars and two small molars. In some cases, the bone tissue in the area of individual holes is absent and then the apex of the roots in contact directly with the mucous membrane of the bottom of the sinus. The lower wall of the middle maxillary sinus is at the level of the bottom of the nasal cavity, but is often located above or below the latter. According to the research data, the bottom of the maxillary sinus in 42.8% of cases is below the lower nasal passage, in 39.3% - on the same level with it and in 17.9% - above it.
Due to the close contact of the lower wall of the maxillary sinus with the roots of the teeth of the upper jaw, inflammation of the apex of the roots can cause inflammation of the maxillary sinus.
By the time of full development of the sinuses there are four cavities, or bays: alveolar, zygomatic, palatal and frontal. Often on the lower wall there are bony protrusions in the form of ridges, which partially, and in some cases completely, divide the sinus into two chambers. Partitions in the maxillary sinus can be either solid or with small holes. The formation of additional maxillary sinuses can also occur due to the ingrowth of one of the ethmoid cells. The capacity of these sinuses in adults ranges from 0.2 to 3.62 cm cube.
Of course, the presence of partitions that divide the sinus into separate parts, is of great practical importance, since due to them the disease can be unrecognized, and washing the sinus during puncture - difficult.
All anomalies of the maxillary sinuses can be detected on radiographs. Radiological abnormalities are detected in 13.3% of patients.
The suction capacity of the mucous membrane and the emigration of leukocytes are regarded as manifestations of the protective function of the shell of the paranasal sinuses.
Blood supply to the paranasal sinuses is provided by the branches of the internal and external carotid arteries, mainly through the orbital, external and internal maxillary arteries. The maxillary sinus feeds mainly on the posterior superior alveolar artery and the anterior superior alveolar arteries - the branches of the maxillary artery.
The outflow of blood from the paranasal sinuses is carried out through the vessels, which abundantly anastomose with each other, with the veins of the nose, face, orbit, and the cranial cavity, with cranial sinuses.
The venous system of the nose and paranasal sinuses is of great importance for the spread of infection.
Lymph outflow from the paranasal sinuses occurs to the deep cervical and pharyngeal nodes. The infection can spread through the lymphatic ducts to the deep sections of the neck and mediastinum.
The innervation of the paranasal sinuses is carried out by the first and second branches of the trigeminal nerve and the fibers of the pterygopalatine node.
In general, the maxillary sinus, like the other paranasal sinuses, protects the nerve structures of the orbit and the anterior cranial fossa from cooling and mechanical damage caused by breathing. In addition, the paranasal sinuses improve the respiratory function of the nose, serve to moisturize the nasal mucosa and perform the resonator function.


Popular
- Breast cancer is curable at any stage.
- The remedy for the cold Sinupret
- Azitrox - official instructions for use
- Chicken-bjaka: allowed antibiotics were found in Russian chicken
- Oral Cancer: Symptoms and Treatment
- Dark and thick blood during menstruation.
- Modern analogues of doxycycline tablets
- Is it possible to die from pneumonia
- What earwax will tell all about your health
- Tussin: instructions for use